Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-03-01
Accepted: 2025-05-25
Published: 2025-07-01
Pages: 142-148
Long-term dental procedures may call for extended mouth opening, which might lead to temporomandibular joint pain, trismus, reduced jaw mobility following surgery, and so on. These problems impair important skills, including chewing, speaking, and maintaining tooth cleanliness, in addition to making one uncomfortable. Physiotherapy is a non-invasive and quick fix aimed to restoring normal jaw function by lowering muscular tension, improving joint flexibility, and thereby boosting the general range of motion. This research explores the efficiency of physiotherapeutic treatments, including thermosapy, manual therapy, passive stretching, and guided jaw exercises, in aiding functional recovery of the temporomandibular joint following significant dental treatments. Patients undertaking physiotherapy reported much improved masticatory ability, less pain, and jaw mobility. The findings underline the probable benefits of adding PT into postoperative therapy strategies to help with faster recovery and improved patient quality of life. Patient education, home-based exercise adherence, and a coordinated multidisciplinary approach combining dental specialists, physiotherapists, and pain experts are guarantees of best therapeutic effects. The study confirms the fundamental component of total dental treatment— physiotherapy inclusion especially in cases when extended treatments raise a patient's functional restrictions of the jaw.
Temporomandibular Joint Disorders are a collection of musculoskeletal and neuromuscular conditions influencing TMJ, masticatory muscles and related tissues displayed by joint pain, clicking sound and limited jaw motion [1]. Many dental treatments require extended mouth opening, which can result in postoperative complications such as trismus, temporomandibular joint dysfunction, and reduced jaw mobility. Mechanical strain on the mastication muscles causes trauma to the TMJ complex or localised, therefore compromising patient quality of life [2]. The TMJ diagnosis requires a multimodal approach that combines clinical assessment with imaging. The therapy aims to prevent additional injury, provide symptomatic relief, and facilitate functional restoration [3]. Patients are sometimes advised to change diet, apply heat and use drugs including NSAIDs and muscle relaxants. The foundation of TMJ treatment is physical therapy [4].
Physiotherapy in medicine is the field intended to restore, preserve, and increase physical capacity and movement. Physiotherapy primarily aims to reduce pain, restore muscular balance, and promote normal jaw mobility [5]. The efficacy of physiotherapy is influenced by patient factors, such as the type of TMJ disorder, the presence of underlying diseases, and the patient's response to treatment. Several treatments, including proprioceptive training, therapeutic exercises to increase muscle movement, muscle strengthening, manual techniques such as passive stretching and joint distraction, ultrasonic and low-level laser stimulation, are applied to reduce discomfort and inflammation in the TMJ [6].
Manual treatment changes the TMJ, releases overactive masticatory muscles, and improves soft tissue flexibility surrounding hands-on techniques. Therapeutic exercises that aim to enhance muscular strength and flexibility through resistance training, as well as controlled mouth opening and closure, help improve jaw function [7]. Patient awareness is one of the factors that most influences the long-term success of treatment. Patients should be taught correct posture and jaw movement to help them stop engaging in parafunctional activities and their detrimental consequences. Methods of leisure and stress management can help lower jaw muscular tension [8]. A coordinated, multidisciplinary approach between dental professionals, physiotherapists, speech therapists, and pain specialists is required to achieve optimal outcomes and ensure patient-centred care [9].
Study Design: This pilot study evaluated the effectiveness of physiotherapy in restoring jaw mobility in individuals who had undergone significant dental procedures and had limited mandibular range of motion, using a prospective, single-group, interventional approach.
Participants: We chose 30 adult patients (ages 18–65) who underwent dental surgeries spanning more than 90 minutes and thereafter complained of pain and difficulty in opening their jaws.
Patients aged between 18 and 65 years.
Underwent dental procedures lasting more than 90 minutes (endodontic therapy under rubber dam, surgical extractions, multiple restorations)
No history of temporomandibular joint (TMJ) dysfunction Patients experiencing jaw stiffness or reduced mouth opening (interincisal opening
History of temporomandibular joint disorders (TMD), systemic muscular disorders, fractures
Patients on medications for muscular disorders
Non-cooperative or unwilling patients
Patients unable to follow physiotherapy protocols Ethical Considerations
The Institutional Ethics Commission approved ethical clearance. Every participant signed a written informed consent before enrolment.
Every member did a thorough baseline evaluation. The first assessment, carried out 24 to 48 hours after surgery, comprised:
Demographic (age, gender, occupation)
Dental operations
Digital calliper maximum interincisal opening (MIO) measurement
On a 10-point Visual Analogue Scale (VAS), reported jaw pain intensity
Functional restriction evaluated with the Jaw Functional Limiter Scale (JFLS-8)
Intervention Under the guidance of a qualified physiotherapist, participants in a controlled two-week rehabilitation program aimed at enhancing mouth muscle
Moist Heat Application: Every session began with moist heat administered to the jaw and perioral area for ten minutes to induce tissue suppleness, increase circulation, and prepare muscles for therapeutic intervention.
Ultrasound Therapy: Therapeutic ultrasonic waves are used to promote deep tissue healing, reduce inflammation, and induce muscular relaxation when applied to the masseter and temporalis areas for five minutes.
Muscle Release Techniques: Manual myofascial release and trigger point treatment targeted the masseter, temporalis, medial and lateral pterygoid muscles, therefore releasing muscular tension and enhancing soft tissue mobility.
Oral Muscle Mobilisation Techniques: Using intraoral and extraoral mobilising techniques, restricted mobility of the temporomandibular joint (TMJ) and associated muscles was treated, therefore increasing flexibility and functional movement.
Exercise Therapy: Oral Muscle Strengthening: Working in a sequential pattern, strength and control in the mouth and jaw muscles evolved:
Regulated jaw opening and closure against resistance.
Lateral deviation, among other exercises.
Retraction and reflection against hand or tool-performance and reducing related discomfort followed.
The intervention strategy consisted of the following elements:
assisted opposition.
Isometric exercises targeting the masseter and buccinator muscles.
Home Exercise Program: Participants received coaching and instruction on a customised home exercise programme, intended to improve consistency of care, promote long-term maintenance, and encourage self-management of symptoms.
Program Duration and Frequency: Over two weeks, therapy sessions are scheduled five times.
Each 30-minute session provided consistent, focused intervention for optimal functional outcomes.
Outcome Measures Assessments were repeated at the end of week 1 and week 2, using the same instruments as the baseline:
Secondary Outcomes: Change in VAS pain score and JFLS-8 scores
Data Analysis
SPSS versions X.X made data analysis possible. Mean ± standard deviation is followed in constant variable presentation. Paired T-tests let one evaluate pre- and post-intervention statistics.
A p-value of 0.05 was considered statistically significant.
Thirty patients were equally divided into two groups: the case group (n = 15), who underwent physiotherapy following long-lasting dental surgeries, and the control group (n = 15), who received regular treatment without physiotherapy.
Baseline demographic and clinical characteristics of groups were identical; initial Maximum Interincisal Opening (MIO), Visual Analogue Scale (VAS) pain ratings, or Jaw Functional Limitation Scale (JFLS-8) scores did not show any appreciable change.
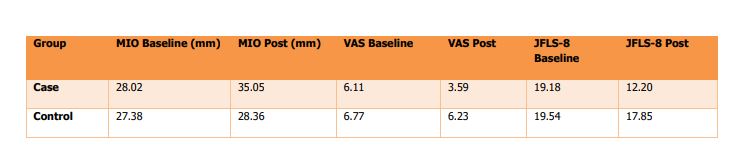
At baseline, the mean MIO in the case group was 28.02 mm (±1.9), while in the control group, it was 27.38 mm. Two weeks later, the mean elevation of the case group - 35.05 mm (±1.6) showed a statistically significant increase in MIO with a p = 0.001. The control group, on the other hand, showed only a tiny, nonsignificant rise to 28.36 mm (±1.7) (p = 0.09).
In the case group, pain levels also improved. From a mean VAS score of 6.11 (±1.0) down to 3.59 (±0.8), the mean dropped 2.52 points (p = 0.001). From 6.77 (±1.1) to 6.23 (±1.0) not statistically significant the control group showed a little decline in pain levels (p = 0.12).
Measuring functional improvement by the JFLS-8, the case group showed notable score changes from a baseline of 19.18 (±2.7) to 12.20 (±2.5) (p < 0.001). Not meeting statistical significance (p = 0.08), the control group declined somewhat from 19.54 (±2.9) to 17.85 (±2.7).
Within the case group, pairwise t-tests confirmed statistically significant increases in MIO, VAS, and JFLS-8 scores—p = 0.001 for each comparison. On the other hand, the control group showed no statistically significant change in any of the studied results. These results highlight the potential benefits of physiotherapeutic intervention in promoting jaw mobility recovery and symptom reduction following major dental procedures Table 1.
| Group | MIO Baseline (mm) | MIO Post (mm) | VAS Baseline | VAS Post | JFLS-8 Baseline | JFLS-8 Post |
|---|---|---|---|---|---|---|
| Case | 28.02 | 35.05 | 6.11 | 3.59 | 19.18 | 12.2 |
| Control | 27.38 | 28.36 | 6.77 | 6.23 | 19.54 | 17.85 |
This retrospective study involving 100 participants helped to determine the outcomes of physical therapy for individuals with temporomandibular disorders. Important clinical results, including maximal mouth opening (MMO), pain levels, and temporomandibular impairment (TMD) scores, were clearly independent of patient age, sex, or number of therapy visits. Considering their demonstrated short-term advantages and minimal risk of adverse effects, the results of this study support non-invasive physiotherapy therapies, such as manual therapy, therapeutic exercise, and patient education, as the first-line treatment for TMD [10]. Another study examined the mandibular range of motion in class III patients, both with and without physiotherapy, after undergoing orthognathic surgery. Patients who had systematic physiotherapy showed a greater increase in jaw mobility than those who did not for six weeks and six months following surgery. These results underlined the likely advantages of early physical therapy in postoperative treatment to enhance functional outcomes. Results and patient recovery in early phases after surgery [11]. M. Gebska et al. investigated the efficacy of therapeutic exercises and manual soft tissue manipulation in a randomised controlled trial in women with myofascial temporomandibular disorders. They discovered that combining therapeutic exercises with myofascial release and post-isometric relaxation greatly reduced pain and enhanced mandibular performance [12]. The results of all the aforementioned research support the effectiveness of physical therapy in controlling temporomandibular issues. Among various patient demographics and clinical environments, conservative treatments, including manual therapy and therapeutic exercises, have consistently demonstrated short-term benefits, including improved mandibular function, reduced pain, and increased range of motion [13]. Early physiotherapy appears to be beneficial in accelerating recovery and optimising clinical outcomes, particularly postoperatively or in conjunction with scheduled rehabilitation programs [14]. Given their low side effect risk, these non-invasive treatments should be first-line therapy options for TMD and be included in comprehensive patient care plans. Future studies with long-term outcomes and tailored therapy approaches will help expand the knowledge base and inform best practices in TMD treatment [15].
While conducting research, developing hypotheses, and gathering data, researchers cannot control every aspect of the research process and are likely to encounter some obstacles along the way. The first limitation alludes to the small sample size. From the given set of data, the researchers cannot hope to assign statistical power and generalize the results. The larger the size of the sample, therefore, the more reliable the results.
Additionally, the researchers are likely to improve the effectiveness of the intervention if the period of study is increased. Prognosis concepts established in physiotherapy suggest that positive outcomes improve with additional time. Perhaps the most notable limitation in the research the researchers did was the study design. Randomization was done into one group, and because of that, the design determined that there was also one group bias in every area, including patient selection and the outcomes. It is very common in studies where researchers are measuring outcomes that focus on self-reporting aspects that are subjective. With two of the outcomes being pain and function, the design also eliminated blinding of participants and assessors, making the results difficult to obtain. Another limitation is that improvements in the most important area of the study, the opening of the jaw, which is the area of interest, are the results measured the study had no follow up steps. Additional limitations included that the findings are also limited to a specific population. Individuals with temporomandibular joint disorders (TMD) were included in the study, even though they are a relevant population, because they were not included.
Lastly, the measuring tools that were used in the study focused on self-report mechanisms and such mechanisms contain bias due to the measure of pain and the level of function based on the self-perception of the individual pain and the individual’s ability to perform movements.
The study doesn’t shy away from its limitations, and the results obtained should be used sparingly, and caution should be used, and the need for more studies of extended durations, and with a more varied population is inescapable to improve on the treatment refinements.
This pilot study supports the therapeutic potential of physiotherapy in restoring jaw mobility, reducing discomfort, and improving functional outcomes in patients with mandibular limitation following prolonged dental procedures. The results of beneficial non-invasive first-line therapies for temporomandibular joint dysfunction reflect an increasing body of evidence supporting physiotherapeutic techniques, including physical therapy, therapeutic exercises, and education, for patients with temporomandibular joint dysfunction. The statistically significant modifications in the case group underscore the need for early, disciplined treatment to improve recovery and prevent ongoing malfunction. These findings confirm the multimodal, patientcentred strategy for improved long-term outcomes and the incorporation of physiotherapy within normal postoperative dental care. Higher sample sizes and long-term follow-up should inspire further studies to validate these conclusions and improve therapeutic plans.