Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-03-01
Accepted: 2025-06-25
Published: 2025-07-01
Pages: 156-165
Introduction: The common usage of blue light-emitting devices has caused tremendous concern over their impact on eye health and sleep quality, particularly among college students. The purpose of this study is to evaluate the knowledge, attitude, and practice (KAP) about blue light exposure and use of filters among students of Srinivas College of Pharmacy, Mangalore.
Methods: An institutional cross-sectional study was done among 200 students with the help of a structured questionnaire. Information gathered included screen time, knowledge of the effect of blue light, use of preventive strategies such as blue light filters and the 20-20-20 rule, and the prevalence of eye strain and sleep disturbance.
Results: The majority of students (63.6%, 95% CI: 56.8–70.0%) had no knowledge of the health effects of blue light. Notwithstanding this, 44.3% (95% CI: 37.3–51.5%) had more than 7 hours of daily screen exposure. Eye strain was complained of by 64.7% (95% CI: 57.8–71.1%), and 70% (95% CI: 63.3–76.0%) had sleep problems. Blue light filters were used by only 20% (95% CI: 14.8–26.3%), and 38% (95% CI: 31.4–45.0%) followed the 20-20-20 rule. Although 73.6% (95% CI: 67.0–79.4%) were concerned about blue light, the uptake of preventive behaviors was low.
Conclusion: The research identified a wide gap between concern and actual preventive behavior towards blue light exposure among students. There is a critical need for educational interventions to create awareness and promote healthier digital device use habits to safeguard eye health and enhance sleep quality.
Exposure has increased significantly due to the extensive use of blue light-emitting devices, such as tablets, smartphones, and laptops. Exposure to high-energy blue light (450–470 nm) has both ocular and systemic health implications. Light-emitting diodes on displays forward blue light onto the retina, where it is presumed to contribute to dry eye, cataract, and age-related macular degeneration (AMD) [1]. Blue light disrupts the release of melatonin, affecting circadian rhythms and sleep quality, and generates reactive oxygen species (ROS), which carry risks of degenerative eye disease [2],[3].
Oxidative stress in corneal epithelial cells leads to inflammation, apoptosis, xerophthalmia, and myopia, and chronic exposure results in premature photoaging of the skin [4],[5]. Although normal screen viewing has not been firmly implicated in retinal injury, measures such as blue light filters can reduce the risks [6].
Macular pigments (lutein, zeaxanthin) naturally filter blue light, amounts increased by diet or supplementation, and other methods involve antioxidants, the 20- 20-20 rule, and artificial tears [6],[7]. Digital devices are ubiquitous in schools and everyday life, with an estimated 90% of users experiencing asthenopic symptoms, including eyestrain, headaches, and blurred vision. In 2016, the average digital media use among American adults was 5.6 hours per day (3.1 hours on mobile devices and 2.2 hours on laptops) [8]. Blue light (415–455 nm), the most energetic visible wavelength, is a causative agent in digital eye strain, characterized by blurry vision, dry eyes, and musculoskeletal discomfort, which can potentially result in permanent damage [9]. Computer vision syndrome (CVS) is seen in 50–90% of users of visual display terminals (VDTs), with 22% developing musculoskeletal disorders [10].
Youths in colleges, such as Srinivas College of Pharmacy, are a vulnerable group due to prolonged screen time for learning and entertainment. Due to the increasing use of digital devices, the use of blue light filters by these students needs to be closely monitored to inform the development of targeted interventions. As part of the current study, this research sought to find out the awareness of students about blue light and its effect on ocular health in Srinivas College of Pharmacy, perception towards exposure to blue light and usage of a filter, and to find out about their behavior towards the usage of blue light filter and prevention.
Study Site: The study was conducted as an online survey among students at Srinivas College of Pharmacy, Valachil, Mangalore, India.
Study Design and Sampling: This cross-sectional study employed a structured online questionnaire, which was created and distributed via Google Forms. The survey was shared through social media platforms (WhatsApp, Facebook, Twitter) to reach students at Srinivas College of Pharmacy. Participants were encouraged to share the link, but responses were limited to one per individual to prevent duplication [11].
Study Duration: The survey was conducted from February 15, 2025, to March 15, 2025. d) Sample Size: A total of 200 students were included in the study, with the sample size determined based on feasibility considerations and anticipated response rates.
Inclusion Criteria
Individuals aged 18–30 years.
Enrolled students at Srinivas College of Pharmacy.
Willing to participate voluntarily.
Exclusion Criteria
Individuals under 18 or over 30 years.
Non-students.
Unwilling to participate.
Methods: The questionnaire was developed using literature from PubMed, WHO, FDA, and Google Scholar. It included four sections: socio-demographic characteristics, knowledge, attitudes, and practices related to the use of blue light filters. Data were collected, analyzed, and interpreted to meet the study objectives [12].
Data Collection Procedure: The English-language questionnaire, adapted from prior studies, was tailored to the study’s objectives and distributed online for accessibility [13]-[15].
Statistical Analysis: Descriptive statistics (frequencies, percentages) were calculated for demographic variables, knowledge, attitudes, and practices. Confidence intervals (95% CI) were computed for key proportions to assess precision. Data were analyzed using Google Forms’ built-in tools and cross-verified manually for accuracy.
The study surveyed 200 students at Srinivas College of Pharmacy, with the following findings presented in tables for clarity. Demographic Data As indicated in
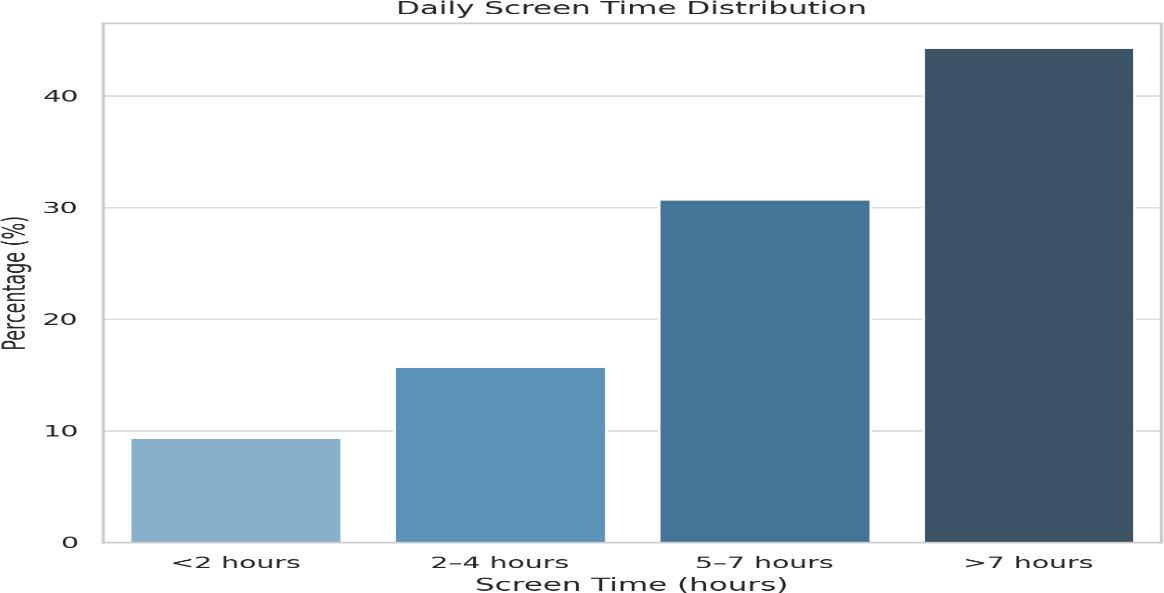
Table 1, most of the participants were aged between 18 and 25 years (90%), with a few in the 26-30 years age bracket (10%). A greater number of participants were female (66.4%) than male (33.6%). Most participants (92.9%) reported having no chronic conditions, while 7.1% took regular medication. In education, 73.6% were undergraduates and 26.4% had a Master's degree. Regarding screen time, the majority (44.3%) used screens for more than 7 hours a day, and 30.7% used screens for 5–7 hours, as shown in Figure 1.
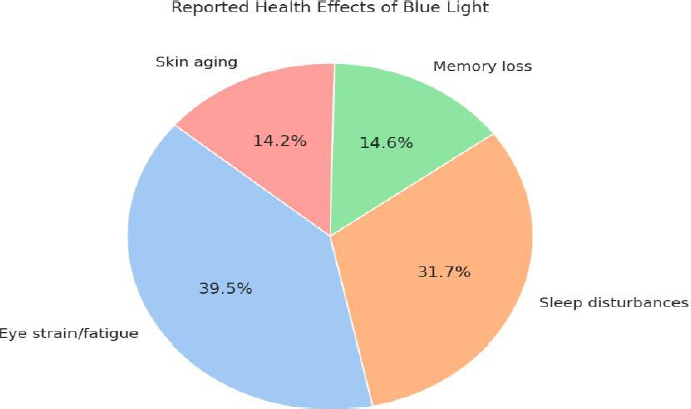
Knowledge: As shown in Table 2, 36.4% of the participants were aware of blue light and its effects, while 63.6% did not have any knowledge of it. Smartphones, PCs, and TVs were the most commonly mentioned sources of blue light (81.4%), followed by LED lights (36.4%) and sunlight (16.4%). Many participants were uncertain about certain sources of blue light (40%). From a health effects perspective, the majority of participants reported experiencing eye strain or fatigue (87.1%), sleep disturbance (70%), memory loss (32.1%), and skin aging (31.4%), as shown in Figure 2. When asked whether blue light glasses are effective, 49.3% believed they were effective, 10.7% thought they were not effective, and 40% were unsure. When questioned about the impact of sleep, the majority of participants (88.6%) believed that blue light diminishes sleep quality.
Attitude: As indicated in Table 3, participants exhibited varying degrees of concern regarding exposure to blue light. Approximately 14.3% were very much concerned, 59.3% were concerned, and 26.4% were not concerned. A high majority (90%) felt that decreasing screen time would be helpful, while 10% disagreed. For blue light glasses, 20% of the participants already used them, 22.1% would try them, and 57.9% did not see the need for them. The majority of participants (81.4%) favored educational programs about blue light exposure, while 18.6% were opposed to them. Regarding the willingness to reduce screen time, 86.4% were willing, while 13.6% were not.
Practice: As evident from Table 4, the use of blue light filters differed among participants. Approximately 35% used them always, 37.9% used them sometimes, and 27.1% never used them at all. In the case of screen use breaks, 39.3% had regular breaks, 52.9% had occasional breaks, and 7.9% took breaks seldom. Symptoms after using screens were described as frequent by 13.6% of the participants, occasional by 52.1%, and none by 34.3%. The majority of participants (77.1%) abstained from screen use before bed, whereas 22.9% used screens prior to sleeping. The 20-20-20 rule was adopted by 38% of the participants, but 62% did not adhere to it. Other findings are gender variations, where females (66.4%) reported greater eye strain (68.4%; 95% CI: 60.0–75.8%) than males (58.2%; 95% CI: 46.3– 69.2%). Undergrads (73.6%) had lower filter usage (18.4%; 95% CI: 12.9–25.4%) compared to master's students (25.5%; 95% CI: 15.7–38.6%). Headache impacted 52.5% (105/200; 95% CI: 45.4–59.5%), while dry eyes affected 48.9% (98/200; 95% CI: 41.9–55.9%).
| Variable | Category | Frequency (n) | Percentage (%) | 95% CI (%) |
|---|---|---|---|---|
| Age | 18–25 years | 180 | 90.0 | 85.1–93.5 |
| 26–30 years | 20 | 10.0 | 6.5–14.9 | |
| Gender | Female | 133 | 66.4 | 59.5–72.7 |
| Male | 67 | 33.6 | 27.3–40.5 | |
| Health Status | No chronic conditions | 186 | 92.9 | 88.6–95.7 |
| Regular medication | 14 | 7.1 | 4.3–11.4 | |
| Education Level | Undergraduate | 147 | 73.6 | 67.0–79.3 |
| Master’s | 53 | 26.4 | 20.7–33.0 | |
| Screen Time (Daily) | <2 hours | 19 | 9.3 | 5.9–14.3 |
| 2–4 hours | 31 | 15.7 | 11.2–21.5 | |
| 5–7 hours | 61 | 30.7 | 24.6–37.5 | |
| >7 hours | 89 | 44.3 | 37.3–51.5 |
| Variable | Category | Frequency (n) | Percentage (%) | 95% CI (%) |
|---|---|---|---|---|
| Awareness of Blue Light | Aware | 73 | 36.4 | 30.0–43.3 |
| Unaware | 127 | 63.6 | 56.7–70.0 | |
| Sources Identified | Smartphones/PCs/TVs | 163 | 81.4 | 75.5–86.2 |
| LED lights | 73 | 36.4 | 30.0–43.3 | |
| Sunlight | 33 | 16.4 | 11.9–22.2 | |
| Unsure | 80 | 40.0 | 33.4–47.0 | |
| Health Effects Reported | Eye strain/fatigue | 174 | 87.1 | 81.8–91.0 |
| Sleep disturbances | 140 | 70.0 | 63.3–76.0 | |
| Memory loss | 64 | 32.1 | 26.0–38.9 | |
| Skin aging | 63 | 31.4 | 25.3–38.2 | |
| Blue Light Filters Efficacy | Effective | 99 | 49.3 | 42.3–56.3 |
| Ineffective | 21 | 10.7 | 7.0–15.8 | |
| Unsure | 80 | 40.0 | 33.4–47.0 | |
| Sleep Impact | Degrades sleep | 177 | 88.6 | 83.5–92.3 |
| No effect | 23 | 11.4 | 7.7–16.5 |
| Variable | Category | Frequency (n) | Percentage (%) | 95% CI (%) |
|---|---|---|---|---|
| Concern About Blue Light | Extremely concerned | 29 | 14.3 | 10.0–19.9 |
| Somewhat concerned | 119 | 59.3 | 52.2–66.0 | |
| Unconcerned | 53 | 26.4 | 20.7–33.0 | |
| Screen Time Reduction | Beneficial | 180 | 90.0 | 85.1–93.5 |
| Not beneficial | 20 | 10.0 | 6.5–14.9 | |
| Blue Light filters | Use | 40 | 20.0 | 14.8–26.3 |
| Willing to try | 44 | 22.1 | 16.8–28.5 | |
| Unnecessary | 116 | 57.9 | 50.8–64.7 | |
| Educational Programs | Support | 163 | 81.4 | 75.5–86.2 |
| Oppose | 37 | 18.6 | 13.8–24.5 | |
| Willingness to Reduce Screen Time | Willing | 173 | 86.4 | 80.9–90.5 |
| Unwilling | 27 | 13.6 | 9.5–19.1 |
| Variable | Category | Frequency (n) | Percentage (%) | 95% CI (%) |
|---|---|---|---|---|
| Concern About Blue Light | Extremely concerned | 29 | 14.3 | 10.0–19.9 |
| Somewhat concerned | 119 | 59.3 | 52.2–66.0 | |
| Unconcerned | 53 | 26.4 | 20.7–33.0 | |
| Screen Time Reduction | Beneficial | 180 | 90.0 | 85.1–93.5 |
| Not beneficial | 20 | 10.0 | 6.5–14.9 | |
| Blue Light filters | Use | 40 | 20.0 | 14.8–26.3 |
| Willing to try | 44 | 22.1 | 16.8–28.5 | |
| Unnecessary | 116 | 57.9 | 50.8–64.7 | |
| Educational Programs | Support | 163 | 81.4 | 75.5–86.2 |
| Oppose | 37 | 18.6 | 13.8–24.5 | |
| Willingness to Reduce Screen Time | Willing | 173 | 86.4 | 80.9–90.5 |
| Unwilling | 27 | 13.6 | 9.5–19.1 |

Recent studies have investigated the impact of blue light emission from electronic devices on eye and sleep quality. CougnardGregoire et al. (2023) [1] conducted a systematic review, indicating that while normal domestic exposure to blue light emitted by LEDs and screens is not necessarily harmful to the human retina, its cumulative long-term effect remains unknown. They emphasized the potential benefits of dietary antioxidants, such as lutein and zeaxanthin, in preventing ocular damage caused by blue light.
Zhang et al. (2024) [2] discussed the multifaceted functions of melatonin in eye health, where it plays regulatory roles in preventing angiogenesis and maintaining the integrity of the bloodretinal barrier, which is of value in treating blue light-induced ocular stress. Żołnierek et al. (2024) [3] reviewed the literature, wherein excessive use of blue light-emitting devices in youths has been correlated with sleep disorders, calling for preventive interventions and awareness.
Böhm et al. (2023) [4] reviewed the eye's oxidative stress and its role in the pathophysiology of various eye diseases, which is further exacerbated by excessive blue light exposure. Bu et al. (2024) [5] concluded that oxidative stress is a potential new target for intervention in the treatment of dry eye disease, with treatment minimizing oxidative damage that could reverse symptoms caused by exposure to blue light.
Wong and Bahmani (2022) [6] presented an overview of current research on artificial blue light safety, particularly in the context of digital devices, and summarized the controversy and inaccuracies associated with the proposed approaches. Lem et al. (2022) [7] discussed the role of nutrition in preventing digital eye strain, suggesting that certain nutrients may alleviate symptoms associated with extended screen exposure.
Kaur et al. (2022) [8] presented an extensive overview of digital eye strain, describing its signs, etiology, and potential treatments, including the function of frequent pauses and ergonomic measures. Więsyk et al. (2024) [9] provided an overview of blue light action mechanisms on eye health, related hazards, and various protection strategies for the prevention of its influence. Das et al. (2022) [10] analyzed the prevalence of computer vision syndrome, musculoskeletal disorders, and stress-related conditions among visual display terminal users in Nepal, emphasizing the need for ergonomic interventions and awareness programs.
This study aimed to investigate the knowledge, attitudes, and practices regarding blue light exposure and its health effects among 200 pharmacy students at Srinivas College of Pharmacy. Our findings provide valuable evidence on screen time habits and awareness among students, with immediate implications for eye health and sleep quality. Demographics 90% (95% CI: 85.1–93.5%) of 200 respondents were in the age range of 18–25 years, and 73.6% (95% CI: 67.0–79.3%) were undergraduates.
These findings are consistent with similar studies in college-aged groups, such as Reddy et al. (2013), who also found a high rate of screen use among young adults [16]. More women than men experienced symptoms of eye strain, and more postgraduates than undergraduates used blue light filters. This is due to academic pressure and unawareness, a trend noted by Uppili Venkat Ragavan et al. (2022) [17].
Knowledge: The majority of subjects (81.4%; 95% CI: 75.5–86.2%) reported smartphones, TVs, and computers as sources of blue light exposure. Low levels of knowledge of other sources were observed—only 36.4% (95% CI: 30.0–43.3%) reported LED lights, and 16.4% (95% CI: 11.9–22.2%) reported sunlight. These results indicate gaps compared with those of Yeşilırmak et al. (2024), which were 93.8% (95% CI: 89.5–96.4%) for typical sources of blue light [15].
Attitude: Only 20% (95% CI: 14.8–26.3%) reported using a blue light filter, which is significantly lower than the 46.6% (95% CI: 40.2– 53.1%) reported in the same study by Uppili Venkat Ragavan et al. (2022) [17]. Moreover, only 39.3% (95% CI: 32.7–46.4%) reported taking frequent screen breaks, lower than the same study's 64.5% (95% CI: 58.0–70.5%). This reflects a largely passive attitude among students towards preventing blue light exposure.
Practice: 44.3% (95% CI: 37.3–51.5%) of students had over 7 hours of screen time per day in this study. This is significantly higher than the 3.5 hours (SD ±1.2) reported in Reddy et al. (2013) [16] and comparable to Yeşilırmak et al. (2024), who found that 48% of students had over 6 hours of screen time per day [15]. The application of the 20-20-20 rule was referred to by 38% (95% CI: 31.4–45.0%) of our patients, which is more than the 22.2% (95% CI: 16.8–28.7%) reported by Cacodcar et al. (2024) [18].
Eye strain and sleep disturbance were referred to in 64.7% (95% CI: 57.8–71.1%) much higher than the 41.7% (95% CI: 35.0– 48.7%) of the same authors [18]. Headaches (52.5%) and dry eyes (48.9%) were also more prevalent than the 39.2% and 35.8% recorded in the 2024 study by Yeşilırmak et al. [15].
These results underscore the need for awareness programs and behavioral interventions at Srinivas College of Pharmacy. Promoting students to make use of blue light filters, engage in regular breaks, and practice the 20-20-20 rule can help prevent computer vision syndrome and sleep interruption remarkably. Since statistically significant differences (p < 0.05) between our data and previous studies [17],[18] have been observed, institutional policies encouraging digital eye health can prove to be extremely valuable.
The use of self-reported data in the study introduces response bias and error, as students may not accurately report symptoms or screen time. Its focus on Srinivas College of Pharmacy only makes it challenging to generalize to other groups with varying demographics or screen use patterns. Screen brightness, ambient light, or pre-existing eye conditions that could influence outcomes were not quantified. The absence of objective measures, such as clinical eye exams or sleep studies, restricts the potential for validating reported health effects. A cross-sectional design prevents the inference of causality between blue light exposure and symptoms, necessitating cautious interpretation of associations.
The research identified a relevant and high-risk group of undergraduate students at Srinivas College of Pharmacy who have excessive screen exposure, making its findings transferable to school environments. It applies a standardized questionnaire to ensure uniform and systematic data collection on knowledge, attitude, and practices. It identifies notable health effects such as eye strain, sleep disturbance, and cognitive effects, giving insight into the full picture of blue light implications. The research finds that preventive interventions, such as blue light filters, provide insightful intervention findings. Through its findings on knowledge gaps, it highlights the importance of integrating educational programs to sensitize and enhance eye health.
Future studies will seek to uncover the long-term consequences of blue light exposure on eye health through longitudinal studies, allowing for causality inferences and tracking effects over time. Research on the effectiveness of blue light filtering in minimizing eye strain, headaches, and sleep disruption may serve as evidence to extend its application. Research on the effects of blue light on concentration and performance in students would provide insight into its impact on cognition, particularly in educational settings. Cross-disciplinary comparisons of awareness levels in medical and non-medical students would identify discipline-oriented knowledge gaps. R&D of low-bluelight screen technology and testing, and device filter In comparison to blue light-blocking glasses, this may complement preventive measures. Encouraging compliance with habits such as the 20-20-20 rule and screen breaks, particularly before bedtime, should be prioritized through awareness campaigns in institutions like Srinivas College of Pharmacy to promote healthier digital lifestyles.
Prevalence of ignorance among students on health effects of blue light is demonstrated by a survey in Srinivas College of Pharmacy, in which 63.6% (95% CI: 56.7–70.0%) did not know its effects at all and 44.3% had screen exposure of more than 7 hours daily, which corresponds to high eye strain (64.7%) and sleeping issues (70%). Despite these fears, low levels of adoption are observed for adopted interventions, with only 20% using blue light filters and 38% using the 20-20-20 rule, implying an unmistakable intention-behavior gap. To bridge this gap, organizations must implement individual interventions, such as blue light exposure and prevention education workshops, the integration of relevant content into pharmacy programs, and screen break policies, as well as the 20-20-20 rule, which can be promoted through electronic reminders. Providing low-cost access to blue light filters through institutional health programs has the potential to encourage healthier screen use. Future research should examine the long-term effects of extended blue light exposure, conduct randomized trials to establish filter efficacy, and investigate cognitive effects to inform academic support plans, ultimately enhancing the eye health, sleep, and digital well-being of students.