Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-04-01
Accepted: 2025-05-25
Published: 2025-07-01
Pages: 178-183
Background: Using materials like metals and fiber-reinforced composites, intra-radicular posts are frequently utilised to reconstruct teeth that have suffered severe loss of coronal structure. Metal posts are less favoured due to esthetic limitations and mechanical incompatibility with dentin. Prefabricated fibre posts often poorly adapt to irregular canal shapes, leading to cement voids and compromised retention. Customising fibre posts to canal anatomy improves fit, reduces cement thickness, and enhances long-term prognosis.
Case presentation: In this case study, a 53-year-old man with a severely decaying, previously endodontically treated upper right second premolar (tooth 15) exhibiting loss of crown structure and a periapical lesion is described as having been successfully managed. Clinical and radiographic evaluation confirmed no pain, swelling, or sinus tract. The tooth was isolated, and retreatment was initiated with canal cleaning, disinfection, and calcium hydroxide dressing, followed by obturation with AH Plus and gutta percha. A post space was prepared, and a prefabricated fibre post was customized using composite resin to replicate canal anatomy. A composite core was constructed after the relined post was light-cured and sealed with dual-cure resin cement. After a week, a zirconia crown was cemented. A three-month follow-up revealed outstanding post-adjustment and full periapical recovery.
Conclusion: Customizing prefabricated fibre posts to match root canal anatomy enhances retention, stress distribution, and preserves radicular dentin. This technique offers a minimally invasive, esthetic, and mechanically superior alternative to conventional posts. Long-term studies are needed to validate its clinical efficacy further.
One common restorative technique for maintaining coronal restorations in teeth with significant coronal tooth structure loss is the implantation of intraradicular posts. Various materials are used to fabricate these posts, including metallic alloys such as stainless steel, titanium, and gold, as well as non-metallic materials like fibrereinforced composites (carbon fibre, glass fibre, and zirconia) and PEEK (polyether ether ketone) [1]. Metal cast posts have fallen out of favour due to their poor aesthetics and high failure rates, primarily because their high modulus of elasticity does not match that of dentin, leading to potential stress concentration or poor force distribution, as well as issues with post preparation and insertion. Additionally, inferior casting quality, such as shrinkage defects, can weaken the post and increase the risk of failure [2]. Prefabricated fibre posts come in definite sizes based on the manufacturing companies. Often, these pre-designed sizes are unable to fit the root canal accurately. Especially in canals that are oval-shaped, cylindrical fibre posts loosely adapt to the walls, giving rise to the increased chances of voids or air bubbles in the cements that are used to lute these posts in the canal [3]. The long-term health of the treated tooth is further jeopardised by these voids, which subsequently weaken and damage the root. Customising the fibre post to the anatomy of the root canal can ensure a thin, uniform film of cement surrounding the post, which results in a reduction of cement volume and creates ideal conditions for post retention [4], as seen in the current case report.
A 53-year-old man with a severely deteriorated upper right second premolar that had undergone endodontic treatment came to the Department of Conservative Dentistry and Endodontics. On examination, 15 showed grossly decayed crown structure with physiological mobility. There was no swelling or sinus, and the patient did not complain of pain or tenderness in the region. Radiographic examination revealed a partially obturated 15 with a periapical lesion Figure 1a.
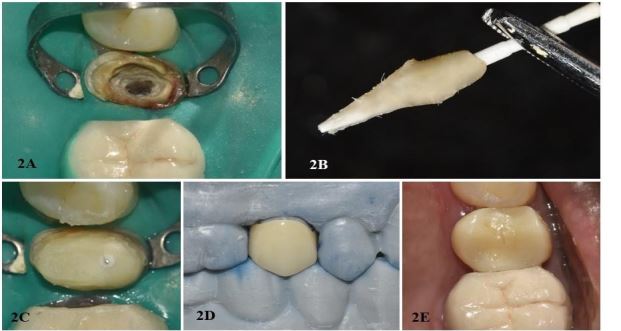
Pulp sensibility tests showed a negative response, and tenderness on percussion was absent. Procedure: Rubber dam isolation was performed after the patient was informed of the treatment plan and provided their consent Figure 2a. An Endo Access bur #2 was used to prepare the access cavity, and a #10 K file and an electronic apex locator were used to determine the working length.
The canal was instrumented using ProTaper Universal Retreatment Rotary files (ProTaper, Dentsply, USA) and 3% sodium hypochlorite (Vishal, India) irrigation. The canal was dried, and calcium hydroxide (Calcipex II, Nippon Shika Yakuhin Co., Ltd., Japan) was placed as an intracanal medicament to enhance the healing of the lesion Figure 1B. After ten days, the patient was rescheduled for additional treatment after the temporary access. The tooth was accessed during the following visit, and the calcium hydroxide medication was washed out with 3% NaOCl irrigation and ultrasonics. Gutta-percha points (GP) (DiaDent Group International, South Korea) and resin-based sealant (AH Plus, Dentsply Sirona, USA) were then used to obturate the canal Figure 1c.
After the sealer had fully cured, the patient was summoned back, the GP was taken out, and a post space was created with a #3 peeso reamer until there was only 4 mm of GP left in the canal. After cleaning, the root canal was dried. To verify the fit, a fibre post (Angelus Reforpost Fibre Glass, Brazil) was chosen and placed inside the canal. This was confirmed with a radiograph Figure 1d.
After 30 seconds of being etched with 37% phosphoric acid (EcoEtch, Ivoclar Vivadent, Switzerland), the post was rinsed and allowed to dry. Using a microfibre tip applicator, silane (Ultradent) was applied to help the composite and fibre post material adhere. The resin composite (Charisma® Smart, Kulzer, Germany) was coated over the post and placed into the canal, closely replicating the canal anatomy. Glycerine was brushed onto the canal to avoid adhesion. After five seconds of intraoral light curing, it was taken out and given an additional 20-second extraoral light cure. Until the post fit snugly inside the canal, this process was repeated incrementally Figure 2b. After conditioning the root canal wall, glue was used. The modified post was coated with silane and then sealed using dual-cure resin cement (Paracore Slow Intro Kit, Coltene, Switzerland).
Then, the core was created over the post and LED-cured to polymerise the composite Figure 2c completely. To ensure that the post and core fit into the canal, a last radiograph was taken Figure 1e. After a week of temporisation, the final zirconium crown was cemented Figure 2d, 2e. A three-month follow-up was conducted. A periapical radiograph demonstrated the healing of the periapical lesion and the custom-modified fibre post and core remaining well-adapted to the post space Figure 1f.











Dentists still face several challenges when it comes to restoring teeth that have undergone root canal therapy, despite continuous advancements in dental technology and materials. The use of fibre posts is a commonly practised treatment modality in teeth with insufficient remaining coronal structure, which cannot provide enough support, strength, and retention for the final restoration [5].
Prefabricated fibre posts were first introduced in the 1990s and have a reported modulus of elasticity (MOE) comparable to dentin [6]. It is thought that the mono-block system design will provide a more even distribution of stressors that the root will experience. This mono-block comprises a dentin-post-core system through dentinal bonding [7].
Fibre posts have several aesthetic advantages, including translucency and improved optical properties. They are chemically inert and biocompatible with the body, and can be easily retrieved in cases of failure. Fibre posts have a better light transmission capacity, high fatigue resistance, excellent insulation, low solubility, and biochemical dissolution resistance [8].
The MOE of dentin (18 GPa) and composite resin (20 GPa) are similar. This enables the core material, resin cement, post, and tooth tissue to form a more consistent restorative system. Therefore, the distribution of stresses along the root is evenly distributed, and the chances of root fracture are considerably reduced [9].
The canal cross-section of single canal premolars can be round, oval, flattened or even C-shaped. As a result, prefabricated fibre posts typically fit loosely in the coronal portion of the root and tightly apically. The post's subsequent size might be short, which could necessitate additional preparation and canal space augmentation by the peeso reamer to achieve a better fit. This, however, would be at the expense of the radicular dentin and the overall strength of the root. Therefore, in such cases, the treatment plan of an “anatomic post” should be considered, i.e., adapting the post to the canal anatomy [4].
Because it fit well apically but loosely coronally, a #1 prefabricated fibre post (Angelus Reforpost Fibre Glass, Brazil) was customised for this case study. Customisation of posts to form a direct anatomic post is usually done in 2 ways. It can be done by recording an impression of the canal directly, by relining the prefabricated glass fibre post with resin composite or by filling the spaces around the main glass fibre posts with accessory fibre posts [10].
When the canal space is quite wide, the second approach is typically used. In this case, the canal was not wide enough; therefore, the first technique was chosen as the treatment plan [11].
Clavijo et al. studied the fracture resistance and mode of failure of bovine teeth restored with various posts. They concluded that direct and indirect composite resin-relined fibre posts, as well as cast metal posts, increased the fracture strength of the root canals [8].
The cast metal post had 100% unfavourable failures; however, the direct and indirect composite relined groups also displayed advantageous failure mechanisms. Hence, it was established that the use of composite relined anatomic posts could be a potential alternative to metal posts [12].
The pushout bond strength of these relined posts was studied by Faria-eSilva et al. (2009) [13], and it was concluded that customising the post with composite improved the retention of fibre posts in all parts of the root canal. In a related study, Rocha et al. (2017) [14] validated these results by comparing the bond strength of resin-modified and non-modified posts, concluding that bond strength was improved by tailoring posts to the canal's morphology, thereby offering a thin and irregular fit. A coating of cement to round the post and disperse the stresses.
Thus, it can be said that personalising the prefabricated fibre post is a straightforward, minimally invasive process that involves only a few more procedures within the same visit. It reduces the need to prepare the root more deeply and shields the dentin, which fortifies the remaining root structure. Furthermore, improved contact between the restorative system and the dentin is created by the hydraulic pressure generated and transmitted to the dentinal walls through the cement. Because blisters in cementing resin can be a source of flaw-initiating sites, this pressure reduces their creation. The pressure increases the penetration of the resin cement into the root dentin tubules and forms a better-quality hybrid layer [15].
To satisfy the inclination towards aesthetic restorations, the adoption of anatomic posts enables a more conservative and long-lasting treatment approach in commonly encountered canal complexities. The tooth was finally restored with a zirconia crown. Its ability to match tooth colour, colour stability, and biocompatibility has made it a popular choice for post-endodontic restorations [16]. Due to its high fracture resistance (4200 N) and modulus of elasticity (208 GPa), zirconia crowns are indicated in severely compromised teeth restored with fibre posts to promote their long-term durability and prevent catastrophic fractures of the tooth [17], [18].
Rehabilitating endodontically treated teeth that have lost a substantial amount of coronal structure is still difficult. This case study demonstrates the clinical effectiveness of modifying prefabricated fibre posts to fit the anatomical shape of the root canal. The direct relining technique using composite resin not only enhanced post retention but also contributed to optimal stress distribution and preservation of radicular dentin. Compared to conventional prefabricated or metallic post systems, the anatomic fibre post technique offers superior esthetics, improved mechanical performance, and a minimally invasive alternative, thereby supporting long-term functional and biological success. Additional clinical research with extended follow-ups is necessary to confirm the results and reaffirm the benefits of this strategy in various clinical contexts.