Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-01-04
Accepted: 2025-03-13
Published: 2025-04-01
Pages: 48-55
Background: Diabetes mellitus (DM) is a common, chronic, debilitating disorder that presents with concomitant oral manifestation that has great implications for oral healthcare. Oral healthcare is often overlooked in the treatment regimen of DM patients. Data regarding the oral disease burden in diabetes patients is vital to plan and implement oral healthcare policies and programs by the concerned authorities. Thus, this study was aimed at determining the oral disease burden in type 2 diabetes mellitus (T2DM) patients visiting a dental hospital in Mysuru city, India.
Methodology: The study had a retrospective cross-sectional observation design with the screening of patients' case records as the data source. Data from three years (2019, 2020, 2021) was considered. Patients' case records of the aforementioned years were screened and known T2DM patients’ records were selected. Data was collected using a structured proforma designed with key variable headings. Detailed demographic data, medical, dental history and clinical findings were recorded from the selected cases. The data was statistical analysis.
Results: Our results showed that T2DM had an overall prevalence of 3.53 %. Individuals of age 40 years and above (86 %) were the most affected. Males were affected more than females in the ratio of 2:1. Periodontal conditions (45%) were the most prevalent oral disease followed by tooth loss (24%) and dental caries (17%). All the other oral conditions together accounted for 14% of the total cases.
Conclusion: Our study highlights the high oral disease burden and the pressing need for oral healthcare management in T2DM patients.
Diabetes mellitus (DM) is a common chronic and debilitating disease. It presents with concomitant oral manifestation that has significant implications for oral healthcare [1],[2]. Type 2 diabetes mellitus (T2DM) constitutes 85- 95 percent of all DM cases [3], [4]. The global spread of DM is accelerating alarmingly.[5] According to the World Health Organization (WHO) predictions, by the year 2030, 366 million adults worldwide will have diabetes, up from 171 million in 2000 [6]. By 2035, the diabetes explosion is expected to hit 592 million people [7], [8]. DM is frequently linked with a high disease burden in developing nations [9]. T2DM is currently in epidemic proportions in India. India accounts for one-fifth of all diabetes cases globally and is frequently known as the diabetes capital of the world.[6] According to the 2009 report of the International Diabetes Federation (IDF), diabetes cases in India were 50.8 million [10]. These numbers have seen a significant surge in recent years to an estimated 101 million cases, according to a study by the Indian Council of Medical Research (ICMR) study published in 2023.11 Studies from various regions of India have shown an increasing prevalence of diabetes in both urban and rural populations due to rapid urbanization. The economic burden of the management of DM and its complications is considerably huge [3]. Compared to healthy individuals, DM sufferers are more likely to experience oral infections and lesions [12]. About 90 percent of DM patients are found to have oral manifestations [8], such as periodontitis, gingivitis, stomatitis, candidiasis, mucormycosis, lichen planus, angular cheilitis, salivary dysfunction, delayed wound healing, burning mouth syndrome, halitosis, dental caries, altered taste, and other neurosensory disorders and tooth loss [5], [8], [12], [13]. Oral healthcare is often overlooked in the regular treatment regimen of DM patients.[12] Data regarding the burden of oral diseases in diabetes patients is essential to planning and implementing suitable oral healthcare policies and programs by the concerned authorities. Reviewing the literature, we found no study on the burden of oral diseases in DM patients undertaken in Mysuru city. Thus, this study aimed to determine the burden of oral diseases in T2DM patients visiting a dental hospital in Mysuru city in Karnataka state, India.
The study was conducted in a dental teaching hospital in Mysuru city, Karnataka state, India. Since the hospital is a tertiary health facility that receives patients from Mysuru city and the surrounding areas, the patient’s demographics primarily reflect those of the entire city. Before initiating the study, ethical clearance was obtained from the Institutional Ethics Committee. The study’s objectives were to record the demographic data and determine the burden of oral diseases in T2DM patients. The study had a retrospective cross-sectional observation design, screening patients’ case records as the data source. Data from three years (2019, 2020, 2021) was considered for the study. All the Patients’ case records of the years above were screened carefully, and case records of known cases of T2DM were selected for further use. Data collection was done using a structured proforma designed with key variable headings. Detailed demographic data, medical and dental history, and clinical findings were recorded from the selected cases. The raw data were entered into a Microsoft Excel spreadsheet for preliminary analysis and exported to SPSS 2022 for further statistical analysis. Data were presented as graphs and frequency tables. Associations were tested using the software.
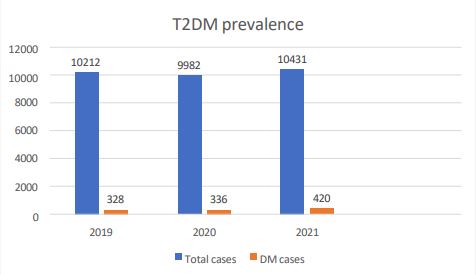
A total of 30,625 case records belonging to the study period (2019-2021) were screened, and out of these, 1084 cases of T2DM were found. This represented an overall T2DM prevalence of 3.53%. The year-wise prevalence of T2DM is as follows: The year 2019 (328 T2DM cases/10212 total patients; prevalence 3.21%;), 2020 (336/9982; 3.36%), 2021 (420/10431; 4.02%). The year-wise trend in T2DM prevalence is similar across the three years. The detailed data is depicted in Figure 1, Table 1.

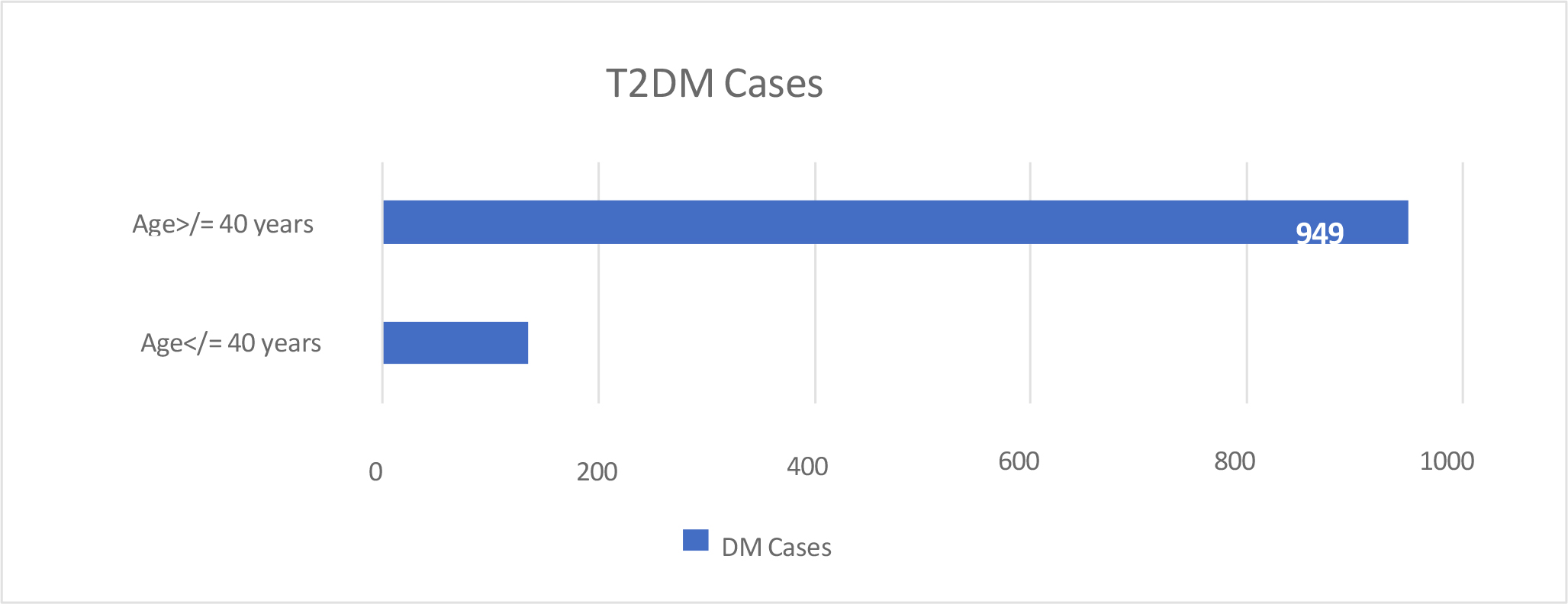
Figure 1 shows the year-wise T2DM prevalence asked on the patient’s age, and graph 2 shows the total number of DM cases based on age. Our results showed a steep increase in disease prevalence above the age of 40, which aligns with the global trend in the age distribution of T2DM.
| Age Group | 2019 | 2020 | 2021 | Total | Percentage |
|---|---|---|---|---|---|
| <40 | 34 | 33 | 68 | 135 | 14% |
| ≥40 | 294 | 303 | 352 | 949 | 86% |
| Year | 2019 | 2020 | 2021 |
|---|---|---|---|
| Male | 210 | 247 | 248 |
| Female | 118 | 89 | 172 |
| Total | 328 | 336 | 420 |
Table 2 shows the year-wise gender distribution of T2DM cases. Graph 3 shows the total T2DM cases based on gender. Our results showed a higher male prevalence in the ratio of 2:1
| Sl no | Oral conditions in T2DM patients | Number of cases | Percentage (%) |
|---|---|---|---|
| 1 | Periodontitis | 398 | 32.52 |
| 2 | Dental caries | 208 | 17.00 |
| 3 | Partially edentulous with chronic generalized periodontitis | 186 | 15.20 |
| 4 | Completely edentulous | 107 | 8.74 |
| 5 | Apical periodontitis | 92 | 7.51 |
| 6 | Gingivitis | 50 | 4.10 |
| 7 | Xerostomia | 35 | 2.85 |
| 8 | Oral candidiasis | 27 | 2.20 |
| 9 | Dentinal hypersensitivity | 25 | 2.04 |
| 10 | Aphthous ulcers | 18 | 1.47 |
| 11 | Periodontal abscess | 18 | 1.47 |
| 12 | Dentoalveolar abscess | 16 | 1.30 |
| 13 | Pericoronitis | 10 | 0.81 |
| 14 | Mucormycosis | 12 | 0.98 |
| 15 | TMJ disorders | 8 | 0.65 |
| 16 | Burning mouth syndrome | 5 | 0.40 |
| 17 | Trismus | 4 | 0.32 |
| 18 | Herpes labialis | 3 | 0.24 |
| 19 | Trigeminal neuralgia | 2 | 0.16 |
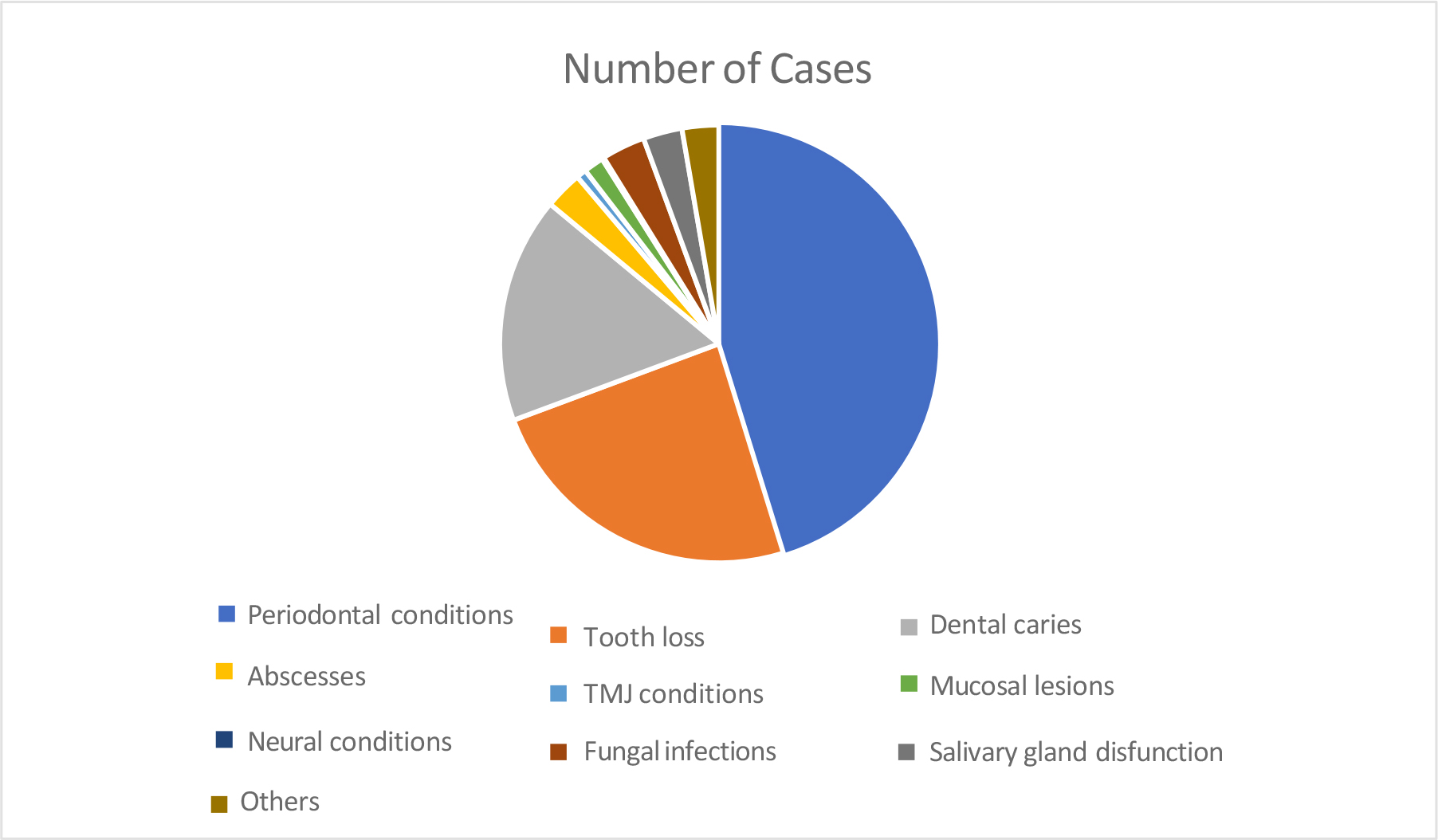
Table 3 shows the distribution of oral conditions in T2DM patients. Figure 3 shows a more concise pictorial representation of the distribution of oral conditions. Our observation showed that periodontal conditions were the most prevalent oral disease, accounting for 45% of total cases, followed by tooth loss (24%) and dental caries (17%). Other conditions accounted for 14% of the oral diseases noted in T2DM patients.
Systemic health impacts oral health, and DM is one of the most prevalent chronic systemic disorders seen in dental practice [7]. Oral symptoms in DM patients indicate poorly regulated blood sugar levels and should be evaluated to detect long-term complications [14]. For the best patient care, the diabetologist and dentist must thoroughly understand the pathophysiology, clinical symptoms, and treatment of DM-related orofacial problems [7]. DM is a public health crisis with immense financial implications due to its chronicity, high and globally rising prevalence, and severe.
Associated complications and the demand for multi-modal treatment [15]. T2DM was the ninth leading cause of mortality in 2017, accounting for more than 1 million deaths. Compared to 1990 data, where it was ranked in the eighteenth position, this surge is frightening [16]. The complications enormously impact DM sufferers’ quality of life and life expectancy [13].
In 2015, the global economic burden imposed by DM was US $ 1.31 trillion [8]. In addition to its financial toll on the national economy and healthcare system, DM frequently results in devastating personal expenditures for patients and their families, including out-of-pocket expenses and lost income from disability and premature death [17]. DM is commonly linked to a high disease burden in developing nations. Estimates of the oral disease burden in diabetes are crucial for allocating community and healthcare resources and promoting actions to halt its rising prevalence [9].
Thus, the primary purpose of this study was to determine the burden of oral diseases in T2DM patients visiting a dental hospital in Mysuru city, Karnataka, India.
Every country is seeing an increase in the number of T2DM patients, with 80 percent of them residing in low- and middle-income nations [18]. A national urban diabetes survey conducted in six major Indian cities showed a diabetes prevalence rate of 12.1%. The highest and lowest prevalence rates among the urban Indian population were reported from Kerala (South India) and Kashmir (north India) states, respectively [3]. The prevalence of rural India by 2015, 2025, and 2035 was estimated to be 7.6%, 10.3%, and 14.7%, respectively [10]. It is also estimated that nearly 57% of Indian adults with diabetes are undiagnosed, which accounts for approximately 43.9 million cases [19].
Our results showed that T2DM had a prevalence of 3.53 % in our study population, which is low compared to the national statistics. This could be because the study period considered was the COVID-19 pandemic years (2019-2021), which saw a downward trend in the overall patient input at the dental hospital compared to previous years.
Our results showed a male predominance and were affected twice more than females. This is in line with the global epidemiological data of diabetes affecting males marginally higher.[20] According to the IDF, men have slightly higher prevalence rates (9.6%) than women (9.0%).[19] Additionally, men are diagnosed earlier in life and with lower levels of overweight/obesity.[20] In our population, 86% of the affected individuals were above 40. This stands true with the well- known fact of the increased incidence of T2DM in the middle and older age group.
Periodontal diseases (PD) were the most prevalent oral diseases among the T2DM patients in our population, accounting for 45% of cases. Our result of the high PD burden in DM is consistent with the available literature, which indicates that PD is the leading oral complication attributed to diabetes, and it is considered to be the sixth complication of DM.[13], [21] Epidemiological studies reveal that DM patients have a three times higher risk of developing periodontitis [7], with the prevalence accounting for 34%- 68%.[8] The prevalence of PD in India is rising at an alarming rate, with incidences of 296 million in 2000 and 363 million in 2015 [6]. There is a bidirectional relationship between PD and DM [8].
Both diseases are more severe and progress more rapidly when they occur together [6]. Proper management of PD is essential for appropriate diabetes control and vice versa [22]. PD is also found to have a strong association with DM complications such as stroke, cardiac failure, nephropathy, and ischemic heart disease [8]. Our findings light the magnitude of the PD burden and the extreme importance of regular periodontal assessment and prompt treatment to maintain optimal periodontal health among DM patients.
Tooth loss was our population’s second most common oral condition, accounting for 24% of cases. According to the literature, an edentulous state is highly prevalent among DM sufferers. A study found that 15.3% of DM patients were completely edentulous, and only 6.4% had natural teeth. The high tooth loss incidence among DM patients is related to PD severity, which leads to alveolar bone destruction, ultimately causing tooth exfoliation [8]. Our finding emphasizes the heightened need for prosthetic rehabilitation among DM patients.
The burden of dental caries was the third-highest in our population, accounting for 17% of cases. Similar to our findings, few researchers report a higher incidence of caries among DM patients when compared to non-diabetics [5],[8]. The relationship between DM and dental caries is complex. Adults with T2DM are more likely to be obese and consume high-calorie, carbohydrate-rich diets. Thus, they may have greater exposure to cariogenic diets. Furthermore, the diminished flow of saliva reported in diabetics is a risk factor for developing dental caries [23]. However, the literature presents no consistent pattern regarding the relationship between dental caries and diabetes [13], [23]. This aspect requires further exploration with a more extensive study population.
Our study noticed an upsurge in the oral mucormycosis cases in our population of T2DM patients as our research gathered data on the COVID-19 pandemic from 2019-2021. During the pandemic, cases of mucormycosis linked to COVID-19 were documented all across the globe, with 70 percent of those occurring in India in diabetics and patients with pre-existing illnesses. The COVID-19 pandemic has also brought to light several vital gaps in dental research and the need for fresh, pertinent data to address the emergency and lessen the impact of future pandemics on dentistry.[24] According to our results, all the other oral conditions associated with T2DM accounted for only 14% of the total cases. Other DM-related oral complications, such as mucosal lesions and xerostomia, demonstrate weaker associations, and inconsistent data have been reported in the literature. [25], [26] DM is a public health emergency, and healthcare professionals play a vital role in its prevention and management [8]. Awareness programs regarding the relationship between DM and oral and general health are the need of the hour [13]. To effectively manage DM and its associated effects on oral health, it is crucial to implement oral health promotion programs, evidence-based management strategies, routine oral screening in people with diabetes, screening for diabetes in high-risk groups in dental clinics, and increased physician and dentist collaboration [7], [8].
Though our study elicited significant findings, several limitations exist, such as the application of a retrospective study design, reliance on patient case records, a limited number of years studied, and the data procured during the pandemic period.
Our results showed that T2DM had an overall prevalence of 3.53 % in our study population. Individuals aged 40 and above (86 %) were the most affected. Males were affected more in comparison to females in the ratio of 2:1. Periodontal conditions (45%) were the most prevalent oral diseases, followed by tooth loss (24%) and dental caries (17%). All the other oral conditions combined accounted for only 14% of the total oral diseases. These findings have significant implications for health policymakers, physicians, dentists, other healthcare professionals, and the public. Oral healthcare is often overlooked in the regular treatment regimen of diabetes patients. Our study highlights the significant oral disease burden and the urgent need for effective oral healthcare management in patients with type 2 diabetes mellitus (T2DM).