Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-01-02
Accepted: 2025-03-13
Published: 2025-04-01
Pages: 56-62
Introduction: Eating behaviour is influenced by stress and psychological factors. Stress eating or emotional eating often leads to the intake of high-sugar food. Diet plays a vital role in developing dental caries, especially sugar. Aim and objective: The objective was to analyse the potential relationship between emotional eating behaviours and caries experience in university-attending students and assess dental caries’ prevalence among university students in Faridabad City, Haryana, India.
Methods: The study involved 510 students between the ages of 18 to 25 years. A questionnaire of 15 questions was designed to assess the emotional eating habits of the students. Dental caries status was evaluated using the WHO criteria for decayed, missing, and filled teeth.
Results: The study revealed that the total emotional eating score among males and females was a significant factor in influencing DMFT scores in the subjects (p<0.001).
Conclusion: Overall, this study showed a statistically significant correlation between Emotional eating and caries experience.
Eating behavior is controlled by many factors including stress and psychological conditions [1]. Stress is “an inharmonious fit between the person and the environment one in which the person’s resources are taxed or exceeded forcing the person to struggle usually in complex ways to cope” [2]. Stress is the main idea in knowing the impact of social and physiological factors on general and oral health [3].
Stress has been a known risk factor for the development of unhealthy emotional eating habits.
That leads to frequent snacking and a higher intake of sugar-containing foods [4]. Such habits are more common in adolescents and college-going students. Adolescence is a critical period related to the development of stress-induced behavioral patterns. Students report stress studying for exams being the most significant source of academic stress leading to disturbed eating behaviors [5]. Also, students are prone to adjust their lifestyle before and during the examination period often in unhealthy habits like increasing their intake of carbohydrates high-fat food and caffeine consumption [6]. According to many studies students under stress are more inclined towards unhealthy eating behaviors. Emotional food intake leads to high-sugar and high-fat food [7]. Diet plays a vital role in the etiology of dental caries especially sugar. Sugars we intake are readily metabolized by bacteria in dental bio-film formation generating acidic by-products that demineralize the tooth structure and dental caries [8].
Also, low saliva levels lead to dry mouth and might further exacerbate the process of demineralization that causes dental caries. Stress leads to lower salivary secretion eventually leading to the increased prevalence of dental caries [9]. The association between stress and dental caries is very well documented. However, the association between stress-related eating behaviors and dental caries is seldom reported especially among young adults.
This study assesses any potential relationship between emotional eating behaviors and dental caries among college students in Faridabad City Haryana India over 4 months.
This cross-sectional study was conducted by choosing 550 students in the age groups between 18 and 25 who were regular students of Manav Rachna University in the city of Faridabad Haryana state in India. The study had taken place from October to January 2023. Based on a pilot test involving 35 students 15 statements were designed in multiple-choice questionnaire format for measuring the emotional eating behavior scored. Based on this a content validity score of 0.8 was calculated. Forty subjects were excluded from the study since they did not complete the questionnaire. Based on this pilot work using the appropriate sample size formula the study was finally conducted with
This cross-sectional study was conducted by choosing 510 participants. Inclusion criteria for the subjects involved subjects attending the selected college between the age group of 18 to 25 only. The exclusion criteria included subjects who gave a positive history of any systemic disease and anybody unwilling to answer the questionnaire. The data were collected through the subjects’ answers to the questionnaire and oral examination to evaluate the status of dental caries. The questionnaire used herein included demographic details and 15 questions framed to gauge the level of emotional eating habits among college students. Every statement was rated on a 5-point answer scale ranging from 1 “Strongly agree” to 5 “Strongly disagree.” Table 1.
WHO caries diagnostic criteria for decayed missing and filled teeth (DMFT) using a mouth mirror and explorer were applied in evaluating the caries condition against the oral examination by a person. The survey participants would only be selected where subjects are willing to complete the questionnaire. Requesting the participant to fill out the questionnaire is made under clear instructions in the company of an examiner in a position to clarify doubts during such a procedure. The questionnaires were filled out and returned to the examiner. Following that a direct oral test was undertaken
| Statement Number | Statement | Options |
|---|---|---|
| 1 | When I feel anxious, I find myself eating. | Strongly Agree (1) / Agree (2) / Neutral (3)/ Disagree (4) / Strongly Disagree (5) |
| 2 | Being with friends who are eating often makes me hungry. | |
| 3 | When I feel upset, I often overeat. | |
| 4 | When I feel lonely, I console myself by eating. | |
| 5 | Fear of failure in a subject makes me hungry. | |
| 6 | When I am under stress, I find myself eating. | |
| 7 | When I have to study, I find myself eating. | |
| 8 | When I’m feeling moody, I tend to eat more food. | |
| 9 | During examinations, I get the urge to eat more than usual. | |
| 10 | When I feel angry or hurt, I eat high- high-carbohydrate food. | |
| 11 | When I feel bored, I distract myself by eating. | |
| 12 | I indulge in comfort eating, especially at night. | |
| 13 | My eating timings are improper especially when I have a lot of work. | |
| 14 | During stressful days I am more prone to unhealthy food. | |
| 15 | When I feel tired, I eat more food. |
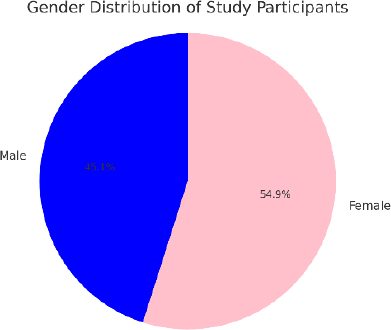
The study included participation by 510 subjects. Two hundred thirty participants were male (45.1%), and 280 were female (54.9%). The subjects ranged from 18 to 25 years of age, with the maximum number of people being 20-22 years of age Figure 1.
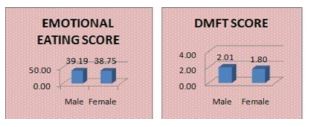
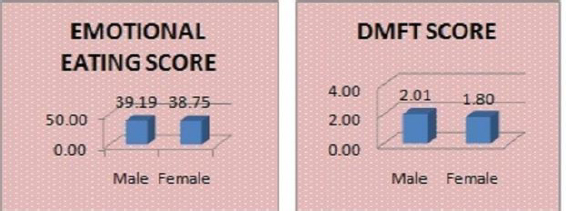
The emotional eating score was calculated according to the evaluation of answers to the 15 statements of the questionnaire using a one-way ANOVA test. Males recorded a slightly higher mean Emotional Eating Score (39.19) than females (38.75) but the difference was not statistically significant (p>0.05). The prevalence of dental caries in the study sample was 79.41% (405). Males had a slightly higher mean DMFT score (2.01) than females (1.80) but the difference was insignificant. (p>0.05) Figure 2.
The analysis was done by using descriptive and inferential statistics. Pearson chi-square test was applied for the categorical data, a paired t-test comparing mean value between the two groups, namely EES and DMFT, and comparison for mean EES values was done by the ANOVA test. The Pearson correlation was applied to perceive relations between the variables. A p-value less than 0.05 is significant at a 95% confidence level. The statistical analysis was performed using SPSS 21.0. In general, the correlation between EES and DMFT scores was intense and of high importance. The study observed that the Emotional Eating Score significantly influenced the DMFT score p<0.001 Table 2.
| Age | Total EES | DMFT Score | |
|---|---|---|---|
| Age | 1 | -0.057 | .103* |
| (0.196) | (0.02) | ||
| Total EES | -0.057 | 1 | -.707** |
| (0.196) | (<0.001) | ||
| DMFT Score | .103* | -.707** | 1 |
| (0.02) | (<0.001) |
*. Correlation is significant at the 0.05 level (2-tailed).
**. Correlation is significant at the 0.01 level (2-tailed).
Convenience sampling was the basis for sample selection in the present study. Previous works have confirmed the possible role of psychological and social factors in dental caries experience though the documentation to support this is sparse. The current study demonstrated a statistically significant correlation between emotional eating behavior and the occurrence of dental caries.
Various cross-sectional studies have previously suggested a positive correlation between overall perceived stress and caries experience in adolescents and young adults [4],[10],[11]. The results of this study were consistent with those of other studies that reported significant relationships between stress factors and caries experience. Emotional Eating is one such stress factor [12],[13]. It is established that daily stress is related to increased desire to eat and hunger-eating motives [14].
Eating disorders encompass a range of conditions including anorexia nervosa bulimia nervosa binge eating disorder avoidant/restrictive food intake disorder other specified feeding and eating disorders (OSFED) pica and rumination disorder [15]-[17].
Although dental caries is one of the most consistently studied oral diseases most published data focus on children and the occurrence of pediatric caries. In contrast studies on caries among adolescents and young adults are fewer. In the present study the mean DMFT score in college-attending students aged 18 to 25 was 1.90.
A significant issue to consider is whether the findings of this study can be generalized to other populations. The sample was by no means representative of the whole population. The site was chosen since it provided sufficient and convenient study subjects and suited the budget within the study’s time frame. The convenience nature of the sample is a significant limitation of the present study. Another limitation of the study was WHO criteria for diagnosing dental caries. This criterion does not allow the diagnosis of initial incipient lesions in enamel and only considers cavitated lesions in dentin.
This study has received a number of valid critiques. First and foremost, the use of convenience sampling when picking subjects means that there is a weaker selection than what is necessary when making the sampling representative of the actual population that the results would pertain to, therefore making the results less generalizable. More so, the study was performed at a single university located at Faridabad, Haryana, and therefore affects the generalizability of the results to other people. Also, the WHO (2004) criteria for diagnosis of dental caries that was used in this study do not consider early caries in the enamel, which would result in dental caries to be less than what the actual situation is. Lastly, by having a total of 510 subjects in the study, which is a good number, the sample size may be representative of the population to a good extent. It is still possible that the study may not capture the diversity present in the student population at the university to enough of an extent.
This study revealed a significant link between emotional eating and the occurrence of dental caries. As a result, clinical practice should aim to educate individuals about stress-induced eating habits as a potential risk factor for developing dental caries. Additionally, it is essential to implement extra preventive measures and counseling strategies tailored for college students. Future studies should explore a broader range of psychosocial factors and biological determinants, focusing on evidence-based research to better understand caries occurrence and its prevalence, particularly among adolescents and young adults.