Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2024-11-29
Accepted: 2025-01-26
Published: 2025-04-01
Pages: 73-79
Alveolar osteitis commonly called as dry socket, alveolalgia osteomyelitis, fibrinolytic osteitis and localized osteitis alveolalgia. It is commonly seen after tooth extraction mainly in third molar extraction. It is a severely painful condition characterized by dislodgement of the blood clot that forms in the socket, leading to exposure of bone. The aproximity in incidence for all routine extraction is 3% and for impacted Mandibular third molar it reaches upto 30%. This review aims to provide an in-depth understanding of dry socket (alveolar osteitis) including it’s pathophysiology, risk factors, prevention strategies and clinical management.
Dry socket (Alveolar osteitis) usually occurs after tooth extraction, particularly after the extraction of impacted third molars. While most extractions heal uneventfully, a subset of patients experience complications. A dry socket (alveolar osteitis) is the most frequent and painful complication. It occurs after the first to third day after extraction. The gingiva is erythematous, swollen, and tender, and the surrounding bone is exposed [1]. It occurs in approximately 3% of extractions and up to 30% of third molar extractions [2],[3].
Predisposing factors include the presence of any infection at the site before and after extraction, smoking, use of oral contraceptives, irradiation, bone disease, underlying pathologies, systemic illnesses such as diabetes mellitus, clotting disorders, and failure to follow post-extraction instructions [4]. Role of bacteria in the breakdown of the clot. An increased incidence of dry sockets supports this. The most commonly detected bacteria were Prevotella, Fusobacterium, Parvimonas, and Peptostreptococcus [5].
Dry socket rarely occurs in patients under 20 years old, likely due to better bone elasticity, improved blood circulation, and enhanced healing capacity [6]. The incidence of dry sockets is mainly seen between the 20 to 40-year age group, with an increased incidence of third molar extraction procedures and a greater prevalence of smoking [5],[6].
The clinical picture typically presents with pain in an empty alveolus, which is observed in most cases. The literature also reveals that pain radiates from dry sockets primarily towards the temporal and ear regions in most cases, and less towards the frontal and ocular areas.
The pathophysiology of dry socket (alveolar osteitis) is due to the premature loss or failure of the blood clot that forms within the extraction site after a tooth is extracted, typically or surgically.
Increased fibrinolysis causes the disintegration of blood clots, resulting in the activation of the plasminogen pathway, which can be achieved by physiological and non-physiological activator substances, i.e., direct and indirect activators. Bacterial products and toxins trigger the indirect activators. It was discovered that active plasmins in the general circulation are inactivated by anti-plasmin [4]-[7]. Brim and this team revealed that the heart, brain, and kidney have less fibrinolytic activity than the uterus tissue and bone [8].
Several mechanisms have been proposed to explain the development of dry sockets. The blood clot may become dislodged prematurely due to mechanical trauma, such as vigorous rinsing, sucking, or forceful coughing. Bacterial invasion in the socket can interfere with clot formation. Common microorganisms associated with dry sockets are Prevotella, Fusobacterium, Parvimonas, and Peptostreptococcus [7].
Inadequate Blood Supply: Factors such as trauma to the blood vessels during extraction, smoking, or any underlying systemic condition can affect blood flow to the socket, reducing the ability to form and maintain a stable blood clot.
Several factors that cause dry socket after tooth extraction is shown in Table 1.
The main hallmark feature of a dry socket is severe pain, often described as throbbing or radiating pain to the ear, eye, or temporal region. Severe, persistent nocturnal pain typically begins 2–5 days after tooth extraction. Other common signs and symptoms include visible bone exposure, halitosis, pain on palpation, a foul taste, low-grade fever, and regional lymphadenopathy [6].
| Smoking | Inhibit clot formation and delay healing |
| Infection | Poor oral hygiene and having local infections like pericoronitis and periodontal disease |
| Oral contraceptive / Menstrual cycle | Alters hormonal levels and increases fibrinolytic activity. |
| Age | The older the patient, the more significant the risk. |
| Difficult extraction | Increase mechanical trauma and clot displacement risk. |
| Previous history of extraction | Increase the risk of dry sockets. |
| Inadequate irrigation | Vigorous rinsing or improper hygiene disrupts clot stability. |
| Remnants of debris and bone /root fragments | Disturbed healing |


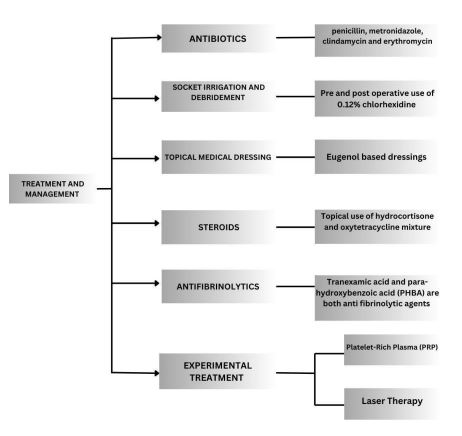
The diagnosis of dry socket (alveolar osteitis) is mainly done clinically. Radiographs are not required unless complications like infection or fracture are suspected. Clinically, suppose the patient has any history of extraction, severe persistent pain starting a few days after extraction, visible bone exposure (empty socket with exposed bone), no signs of infection (no pus), or tenderness on palpation. In that case, these clinical findings are diagnostic of dry sockets [3]-[5]. Managing dry socket (alveolar osteitis) focuses on relieving pain, controlling infection, and promoting healing. Systemic antibiotics are given, like penicillins, metronidazole, clindamycin, and erythromycin [8]. The routine use of systemic pre- and postoperative antibiotics can lead to bacterial strain resistance, hypersensitivity, and disruption of host commensalism [9].
Tetracycline is applied locally in the form of powder. Pre- and post-operative use of 0.12% chlorhexidine solution can irrigate the socket and decrease the frequency of dry socket. A 50% reduction in the occurrence of dry socket is discovered with 0.12% chlorhexidine for 30-second prerinsing of patients [10].
Topical medicinal dressings, such as Eugenol-based dressings containing eugenol, butamben, and iodoform, are also used to manage pain and inflammation in dry sockets. These dressings provide symptomatic relief and should be replaced every two days for optimal efficacy. Studies indicate an 8% incidence of dry sockets when packed immediately compared to 26% in unpacked sockets [11]. Some steroids, such as hydrocortisone and oxytetracycline mixtures, are used topically, which can decrease the chances of developing a dry socket (Alveolar osteitis) after extraction [12]. It was found that corticosteroids can reduce postoperative complications but fail to prevent the development of dry sockets [7]-[9].
Other interventions like antifibrinolytics include tranexamic acid and para-hydroxybenzoic acid (PHBA), these are anti-fibrinolytic that act decrease both plasma and plasminogen. With the use of tranexamic acid and parahydroxybenzoic acid the occurrence of dry socket (Alveolar osteitis) can be prevented [emphasize [13]]. Sutures along with local hemostatics were applied and the combination used of local hemostatics and primary closure and sutures and tranexamic acid can decrease the occurrence dry socket (Alveolar osteitis) [14].
Some adjunctive and experimental treatments are PRP and Laser therapy. In the management of dry socket, pain alleviation and the enhancement of tissue healing associated with the use of PRP are beneficial. The use of PRP and PRF (platelet-rich fibrin) applied to a healing sponge over the extraction site is a significant factor in the healing process and a substantial factor in the reduction in the occurrence of dry socket [6]. Laser Therapy includes Low-level laser therapy (LLLT), which is also pain and inflammation noninvasive. LLLT improves the healing of wounds by reducing inflammation in the tissue of the targeted area. LLLT is applied post continuous mode diode laser irradiation of the socket (808 nm, 100, 60 sec, 7.64 J/cm2) [10]-[14].
The standard review shows diverse papers, including eight review papers and six research papers. All 14 articles indicate that alveolar osteitis is a common post-extraction complication. As we see, several causes of dry sockets include smoking, infection, contraceptive use, menstrual cycle, age, traumatic extraction, a previous history of extraction, inadequate irrigation, remnants of debris and bone, and root fragments. The management of dry sockets focuses on relieving pain, controlling infection, and promoting healing. Prescribed medications include antibiotics, antifibrinolytic agents, and topical treatments. Advanced interventions, such as platelet-rich plasma, platelet-rich fibrin, and laser therapy, may also be used [6]. To mitigate the occurrence of dry sockets, pre-extraction assessments, as well as preventive measures, should be undertaken prior to the extraction. This can be done by advising patients to refrain from smoking before and after the surgery and through copious irrigation of the socket.
One of the most interesting observations that can be made is the difference in the incidence of dry sockets as it relates to age. This is because patients that are in the age range of 20-40 anos are the ones that are more affected by this condition. This is likely related to the fact that this age group is more likely to have their third molars extracted, and also more likely to be smokers. Younger patients are also considered to be at less risk, which is likely related to the literature describing younger patients as having better bone that is more elastic, and better overall healing. A broad range of risk factors have also been noted in the review, and these include systemic risk factors such as diabetes mellitus and disorders related to coagulation. Osteopathies, the use of oral contraceptives, and smoking also have high risk factors for this condition. This emphasizes the need to perform a preoperative assessment in a thorough and comprehensive manner in order to improve the outcome for the patients. One of the most important factors in this condition, from a clinical point of view, is that of pain. This is usually pain that is very severe that does not resolve for some time, and pain that is also radiating from the affected area. There can also be presence of bone that is exposed, and an unpleasant taste is also associated with this condition. Because of these features, along with a comprehensive history and physical examination, it becomes easier to make a diagnosis, which should be the main concern in clinical care.
This allows for less need for imaging unless it is to look for some complications, which are most likely to be infection or fracture.
This review examines multi-strategic management options that balance out symptom management, infection control, and improving overall recovery. Topical solutions, such as eugenol dressings and tetracycline powder, work to minimize pain and inflammation. Preoperative chlorhexidine mouth rinses enhance antimicrobial control and significantly reduce dry socket occurrence [10]. However, the systemic antibiotics as standard treatment are controversial because of the potential for resistant strains and adverse alterations to the oral microbiome.
Dental extraction carries a risk of complications, especially in patients undergoing removal of their impacted third molars. One such complication is Dry Socket, which is considered a self-limiting condition, although alveolar osteitis has aetiological factors that are numerous. In order to provide patients suffering with this condition with better clinical care, clinicians require knowledge of the dry socket condition including the risk factors and the available strategies to mitigate the condition dry socket. Where the condition of the dry socket is manages with the objectives of reducing pain and infection, and fostering repair, the clinicians should consider that improving the condition requires active pain control and infection containment as the key objectives of management ply the greatest potential in improving the condition. More research, particularly research in improving tissue repair with the use of dressings incorporating nanotechnology, and enhanced formulations of PRP, plasma rich in growth factors, is needed. There is no doubt that early intervention and resolution of the condition is a clinical imperative if pain and the other sequelae of the condition are to be optimally controlled. Socket irrigation with 0.12% chlorhexidine followed by placement of a paincontrolling medicinal dressing which is then followed up is the standard practice. The condition is a function of the morbidity and the persistence of the condition.