Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-01-04
Accepted: 2025-03-17
Published: 2025-04-01
Pages: 95-110
SARS-CoV-2 is a single-stranded RNA-enveloped virus. It was the principal causative agent for the global pandemic of COVID-19. Amongst the plethora of systemic and orofacial manifestations from COVID-19 disease and anti-SARS-CoV 2 vaccines, the neurological presentations in the orofacial region have been peculiar. This systematic review aims to document these presentations and understand their association with the viral agent and its vaccines. The research was carried out by electronic searching of database records from December 2019 till December 2023.
This review observed neurological manifestations in the oro- facial region due to COVID-19 disease and anti-SARS-CoV 2 vaccines. The most commonly observed manifestations were trigeminal neuralgia from the COVID disease and Bell’s palsy from the COVID vaccines. The reported number of cases came out to be 6% for bell’s palsy, 90% for trigeminal neuralgia, 1.50% glossopharyngeal neuralgia and 0.01% cases of headaches secondary to neuralgias.
Neurological symptoms are usually associated patients with COVID-19. Trigeminal neuralgia was the most commonly observed neurological symptom in this disease. A deeper insight would enhance oral physicians’ preparedness to improve the screening for accurate diagnosis, appropriate management and concise reporting to the Ministry of Health and Family welfare.
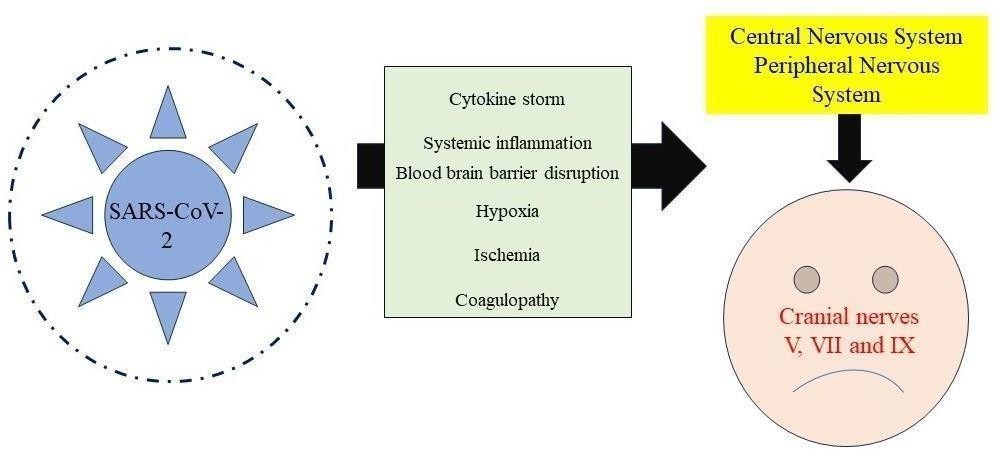
One of the most lethal worldwide pandemics a highly contagious infectious disease emerged in December 2019 causing extensive disruption across seven continents. COVID-19 is the name the World Health Organization gives to the disease derived from the novel Coronavirus which is accountable for its causes. This virus is the seventh virus to infect humans and is a member of the beta-coronaviridae family [1]. SARS-CoV-2 is an enveloped virus composed of single-stranded RNA. Researchers characterized the entire genome structure as 29881 bp in length which encodes 9860 amino acids. SARS-CoV-2 infiltrates the host by binding its spike protein to ACE2 receptors [2]. The proposed mechanisms for COVID-19 infection include (a) direct cellular damage; (b) downregulation of ACE2 receptors which results in dysregulation of the renin-angiotensin system leading to reduced cleavage of angiotensin I and II; (c) thrombo inflammation as a result of endothelial cell damage; and (d) dysregulation of the immune response and hyper inflammation caused by viral inhibition of interferon signaling depletion of T- lymphocytes and increased production of proinflammatory cytokines particularly IL-6 and TNFα [3]-[5]. Few researchers proposed the mechanisms. Many collaborative international investigations after the COVID-19 pandemic have facilitated the rapid advancement of effective vaccinations. The primary vaccinations were implemented in early 2021 to alleviate the pandemic. Additionally, nearly 68.2% of the sector’s population has received a comprehensive vaccination against this disease [6].
Researchers. have outlined four primary methodologies that are employed in the development of anti-SARS-CoV-2 vaccines.
(a) Vaccination based on nucleic acids (DNA or mRNA) (b) Viral vector (replicating or non- replicating) (c) Live inactivated (or attenuated) virus (d) Protein (spike protein or its constituents) In nucleic acid and adenovirus-based vaccinations the synthesis of viral proteins is initiated when segments of the viral mRNA or genome infiltrate human cells. Ultimately these viral proteins are recognized as antigens and induce the production of antibodies. In vaccines that contain inactivated viruses or viral proteins viral debris and proteins function as antigens that stimulate the immune response [7]-[9].
11 potential vaccines for COVID-19 had been authorized for mass immunization by the World Health Organisation as of November 2021 following the successful completion of phase 3 clinical trials. However, the essential phase 4 clinical trials were not included. Researchers have demonstrated that the efficacy of vaccines is contingent upon the results of phase 4. The objective of this review is to provide a comprehensive overview of the oro-facial neurological symptoms that are linked to COVID- 19.

The study used predetermined inclusion and exclusion criteria which involved an electronic search of database records from the previous three years. Case series case reports and observational studies such as case-control studies cohort studies and cross-sectional studies were included in the inclusion criteria. The exclusion criteria included unpublished data studies with only abstract availability letters to the editor and papers published in languages other than English—the specific PICO query aimed to investigate patients with COVID-19 exhibiting oro- facial neurological symptoms. There was no intervention or comparative group in the study. The primary goal was to examine the correlation between SARS-CoV-2 infection and clinical presentations in the oral cavity and evaluate cases of neurological and oro-facial symptoms in patients diagnosed with COVID-19 and those linked to anti-COVID vaccines. The review period was from December 2019 to December 2023. The study aimed to examine the neurological consequences of COVID-19 and its associated vaccines in the oro-facial region. The objectives included the investigation of the neurological manifestations associated with various anti-SARS-CoV-2 vaccinations in the oro- facial region including their incidence and duration as well as the comprehension of the forms and prevalence of COVID-19 that affect the oro-facial region.
The search technique employed electronic databases such as PubMed Scopus and Google Scholar and employed terms such as COVID-19 disease orofacial manifestations neurological manifestations vaccinations and SARS-CoV-2. The search period was from December 2019 to July 2023.
| Author | Country | Study Type | No of Cases | Facial Palsy Characteristics | COVID-19 Related Symptoms |
|---|---|---|---|---|---|
| Lima et al. | Brazil | Case series | 8 | Age: 25 - 50 years Gender: 7 females and 1 male Affected site: 4 cases each of right and left side | Cough, malaise, sore throat, nausea, fever, right-sided ageusia of tongue and anosmia |
| Honma et al. | Japan | Case report | 1 | Age: 35 years Gender: Female Affected site: Right | Cough, malaise, sore throat, nausea, fever, right-sided ageusia of tongue and anosmia |
| Goh et al. | Singapore | Case report | 1 | Age: 27 years Gender: Male Affected site: Left | Myalgia, cough, fever, dysgeusia, left-sided throbbing headache, and conjunctival infection |
| Figueiredo et al. | Portugal | Case report | 1 | Age: 27 years Gender: Male Affected site: Left | None |
| Caamaño et al. | Spain | Case report | 1 | Age: 27 years Gender: Male Affected site: Left | Fever, cough, and pneumonia |
| Muas et al. | Spain | Case report | 1 | NA | Fever, significant asthenia, headache, myalgia, nausea, headache, odynophagia, and vomiting |
| Mangantoni et al. | Italy | Case series | 3 | Age: 27 years Gender: Male Affected site: Left | Fever, dyspnea, hyposmia, ageusia |
| Khaja et al. | USA | Case report | 1 | Age: 27 years Gender: Male Affected site: Left | Ageusia |
| Sancho-Saldanha et al. | Spain | Case report | 1 | NA | Fever, dry cough, and dyspnea |
| Theophanous et al. | USA | Case report | 1 | Age: 35 years Gender: Female Affected site: Right | None |
| Dahl et al. | Norway | Case report | 1 | NA | Fever, headache, dyspnea |
| Egilmez et al. | Turkey | Retrospective cohort | 8 | Age: 35 years Gender: Female Affected site: Right | Pneumonia |
| Corrêa et al. | Brazil | Case series | 4 | Right-sided facial muscle weakness and right lagophthalmos | Vertigo, mild dyspnea, and fever |
| Chan et al. | Canada | Case report | 1 | Age: 35 years Gender: Female Affected site: Right | None |
| Ozer et al. | Turkey | Case report | 1 | NA | Fatigue, chills, and myalgia |
| Neo et al. | Singapore | Case series | 2 | NA | None |
| Mackenzie et al. | USA | Case report | 1 | NA | Ageusia, anosmia, headache, malaise, and cough |
| Bastola et al. | Nepal | Case report | 1 | Age: 35 years Gender: Female Affected site: Left | Mild dry cough and hypoxia |
| Hookham et al. | UK | Case report | 1 | Age: 35 years Gender: Female Affected site: Right | Fever, diarrhea, vomiting, mild headache, intermittent right-sided chest pain, myalgia, lethargy, and conjunctival injection |
| Kheder et al. | Egypt | Case report | 2 | Age: 35 years Gender: Female Affected site: Left | Fever, dysphagia, and vomiting |
| Kumar et al. | India | Case report | 1 | NA | Fever, dysgeusia, and anosmia |
| Aasfara et al. | Morocco | Case report | 1 | Age: 35 years Gender: Female Affected site: Right | Vertigo, nausea, and vomiting |
| Paybast et al. | Iran | Case report | 1 | Age: 35 years Gender: Female Affected site: Bilateral | Band-like headache, dysphagia, and mild dizziness |
| Bigaut et al. | France | Case report | 2 | NA | Cough, anosmia, ageusia, and diarrhea |
| Ottaviani et al. | Italy | Case report | 1 | NA | Acute fatigue, mild fever, and cough |
| Casas et al. | Spain | Case report | 1 | Age: 35 years Gender: Female Affected site: Right | Malaise, fever, dry cough, and headache |
| Hutchins et al. | USA | Case report | 1 | Age: 45 years Gender: Female Affected site: Right | Fever, cough, dyspnea, diarrhea, nausea, headache, nasal congestion, and hypoxia |
| Abolmaali et al. | Iran | Case series | 3 | Age: 25 years Gender: Female Affected site: Left | Fatigue |
| Oke et al. | USA | Case report | 1 | NA | Fever and body aches |
| Derollez et al. | France | Case report | 1 | NA | Fatigue, myalgia, chills, and moderate cough |
| Hasibi et al. | Iran | Case report | 1 | NA | Fever, malaise, dry cough, and anorexia |
| Taouhlar et al. | Morocco | Case report | 2 | NA | Dyspnea |
| Kaplan et al. | USA | Case report | 1 | Age: 35 years Gender: Female Affected site: Left | Fever, chills, headaches, fatigue, myalgia, and weakness |
| Kerstens et al. | Belgium | Case report | 1 | NA | Ageusia |
| Kakumoto et al. | Japan | Case report | 1 | NA | Fever and dysphagia |
| Al-Mashdali et al. | Qatar | Case report | 1 | NA | Fever, cough, watery diarrhea, vomiting, conjunctivitis, and abdominal pain |
| Judge et al. | USA | Case report | 1 | NA | Cough, fever, and chills |
| Tran et al. | USA | Case report | 1 | NA | None |
| Silveira et al. | Brazil | Case report | 1 | NA | Fever, dry cough, and dyspnea |
| S. No. | Authors and Year | Country | Condition | Cases |
|---|---|---|---|---|
| 1 | Taşlıdere B et al. (Mar 2021) | Turkey | Melkersson-Rosenthal Syndrome | 1 |
| 2 | Namavarian A et al. (Aug 2022) | Turkey | Facial Nerve Palsy (without GBS) | 37 |
| 3 | Namavarian A et al. (Aug 2022) | Turkey | Facial Nerve Palsy (with GBS) | 29 |
| 4 | Nguyen BQ, Alaimo DJ | - | Glossopharyngeal Neuralgia | 1 |
| 5 | Omer Karadas et al. (June 2020) | - | Glossopharyngeal Neuralgia | 9 |
| 6 | Omer Karadas et al. (June 2020) | - | Primary Headaches | 64 |
| 7 | Omer Karadas et al. (June 2020) | - | Trigeminal Neuralgia | 9 |
| S. No. | Author | No of cases |
|---|---|---|
| 1 | Abrishami et al. (2020) | 69 |
| 2 | Aggarwal et al. (2020) | 68 |
| 3 | Atum et al. (2020) | 58 |
| 4 | Chen et al. (2020) | 23 |
| 5 | Guan et al. (2020) | 4 |
| 6 | Güemes-Villahoz et al. (2020) | 35 |
| 7 | Hong et al. (2020) | 15 |
| 8 | Karimi et al. (2020) | 2 |
| 9 | Lan et al. (2020) | 3 |
| 10 | Landecho et al. (2020) | 6 |
| 11 | Lee et al. (2020) | 4 |
| 12 | Loffredo et al. (2020) | 13 |
| 13 | Lomi et al. (2020) | 9 |
| 14 | Ma et al. (2020) | 4 |
| 15 | Marinho et al. (2020) | 12 |
| 16 | Meduri et al. (2020) | 3 |
| 17 | Öncül et al. (2021) | 16 |
| 18 | Perlman et al. (2020) | 218 |
| 19 | Rokohl et al. (2020) | 9 |
| 20 | Seah et al. (2020) | 5 |
| 21 | Sindhuja et al. (2020) | 3 |
| 22 | Sun et al. (2020) | 2 |
| 23 | Tostmann et al. (2020) | 1 |
| 24 | Wu et al. (2020) | 4 |
| 25 | Xia et al. (2020) | 12 |
| 26 | Xu et al. (2020) | 2 |
| 27 | Zhou et al. (2020) | 1 |
| S. No. | Author | Neurological complication of Bell’s Palsy | Country | Vaccine type | Duration after vaccination |
|---|---|---|---|---|---|
| 1 | Shemer et al. (a report of 9 cases) | Bell’s Palsy | Israel | BNT162b2 SARS-CoV-2 vaccine | 4–30 days after the first dose, 2nd dose |
| 2 | Repajic et al. | Bell’s Palsy | USA | Pfizer-BioNTech COVID-19 mRNA vaccine | 36 hr after the second dose |
| 3 | Colella et al. | Bell’s Palsy | Italy | mRNA BNT162b2 | 5 days after the first dose |
| 4 | Martin-Villares et al. | Bell’s Palsy | Spain | Moderna COVID-19 vaccine | 2 days after the second dose |
| 5 | Nishizawa et al. | Bell’s Palsy | Japan | Ad26.COV2.S vaccine | 20 days after vaccination |
| 6 | Gómez de Terreros et al. | Bell’s Palsy | Spain | Pfizer-BNT162b2 mRNA vaccine | 9 days after vaccination |
| 7 | Burrows et al. | Bell’s Palsy | UK | The first and second doses of Pfizer-BioNTech COVID-19 vaccine | Right palsy, five hours. Left palsy after 2 days |
| 8 | Obermann et al. | Bell’s Palsy | Germany | First dose of SARS-CoV-2 mRNA vaccine Comirnaty (BNT162b2, BioNTech/Pfizer) | 2 days after vaccination |
| 9 | Iftikhar et al. | Bell’s Palsy | Qatar | Second dose of mRNA-1273 vaccine | 1 day after vaccination |

Bell’s palsy (BP) is an idiopathic sudden paralysis of the facial nerve. Varicella Zoster Epstein-Barr virus Cytomegalovirus and Herpes Simplex Virus-1 are among the numerous viruses responsible for the condition. The research has identified multiple instances in which COVID-19 patients exhibit Bell’s palsy as the solitary primary neurological manifestation of the virus. The authors have identified SARS-CoV-2 as one of the causal agents as it emerged within eighteen days of coronavirus infection. Thirty-two germane publications from five countries worldwide were identified in this review. Unilateral Bell’s Palsy was observed in five patients while bilateral Bell’s Palsy was observed in three patients. Bell’s palsy was identified as the primary manifestation in most instances. The development of ganglioside auto-antibodies was observed during the m The sudden onset and cessation of unilateral acute facial pain characterizes trigeminal neuralgia (TN).
Innocuous stimuli may induce episodes and their distribution is restricted to one or more subdivisions. The estimated prevalence is 0.07%. Researchers reported the existence of a direct pathway from headache and facial pain to COVID- 19 diagnosis. In a retrograde manner the virus directly infiltrates and spreads to the central nervous system. This is the result of the attachment of SARS-CoV-2 to the surface receptors of angiotensin-converting enzyme type 2 which are situated in the trigeminal nerve terminals of the nasal cavity. Few researchers also reported that a cytokine storm indirectly activates the trigeminal-vascular system increasing systemic inflammatory indicators including calcitonin gene- related peptide.
The authors found that headaches were a symptom that appeared on the fourth day after the onset of viral symptoms. However, it was not linked to illness. Hemi-cranial involvement was determined to be prevalent. Patients reported that their pain was exacerbated by physical activity or head movements. Two individuals reported craniofacial irritation that was not associated with trigeminal nerve involvement.
The direct relationship between TN and SARS-CoV has not yet been established. As a result, researchers documented five instances of neuropathic pain in their December 2021 series on the neurological manifestations of COVID-19. However, they did not provide any information regarding the afflicted nerve regions or the nature of the pain [35]-[40].
Javier Mozilla Gill et al. identified 22 instances of trigeminal neuralgia that emerged within three months following COVID-19 infections in January 2022 after examining cases of COVID-19 diagnosed with trigeminal neuralgia [41]-[45].
The COVID-19 vaccination can affect cranial and peripheral nerves leading to side effects. These include Bell’s palsy (facial nerve palsy— seventh cranial nerve) abducens nerve palsy (lateral rectus ocular muscle nerve palsy—sixth cranial nerve) visual impairment olfactory dysfunction auditory issues Guillain–Barré syndrome (GBS) small fiber neuropathy Parsonage-Turner syndrome and Herpes Zoster.
In May 2022 Alexander Muacevic and colleagues proposed that immunomodulation the consequence of molecular mimicry is a mechanism for Herpes Zoster following COVID-19 immunization. They observed functional impairment of CD4+ T cells as well as a decrease in the number of CD3+ and CD8+ lymphocytes. Bell’s palsy and small fiber neuropathy were frequently observed in conjunction with mRNA-based vaccinations which resulted in Herpes Zoster. Anterograde axonal transport towards the periphery is induced by reactivation. MRNA-based vaccinations may increase the risk of Herpes Zoster.
In August 2022 A. Riad reported a Ramsey Hunt Syndrome (RHS) case after the Pfizer immunization. Consequently, RHS leads to vestibulocochlear neuropathy glossopharyngeal nerve neuropathy and facial nerve palsy. As a consequence, it leads to auditory impairment facial paralysis and tongue numbness [46]-[50].
There have been documented cases of intracerebral hemorrhage cerebral venous sinus thrombosis ischaemic stroke and thrombocytopenia following the administration of COVID-19 vaccines particularly those based on adenoviruses as a result of immune system activity. This issue is primarily caused by vaccinations that are derived from adenoviruses. This is the consequence of the transfer of nucleic acids that encode the viral spike (S) protein.
The viral genetic elements infiltrate the extracellular ‘matrix attaching to factor four platelets and inducing an autoimmune response. This pathogenesis is proposed as a potential cause of neurological issues associated with insufficient immunization such as documented central nervous system demyelination (CNS) [51]-[56]. Localized demyelination within the trigeminal nerve (CN V) root is one of the proposed hypotheses for trigeminal neuralgia (TN). Nerve root compression similar to a neurovascular conflict typically initiates the process. Glossopharyngeal neuralgia is generally characterized by intermittent acute piercing pain that affects the ear tonsillar fossa base of the tongue or area beneath the angle of the mandible.
Nguyen B Q [40] identified systemic hypoxemia as a supplementary etiological component of neuralgias. Functional neurological disorders (FNDs) are neurological conditions that impede sensory or motor function. Conventional brain diseases or other medical conditions cannot explain this. Functional Movement Disorder (FMD) is a common symptom of Functional Neurological Disorder (FND) [57]-[63]. It is characterized by various altered movement symptoms including dystonia tremors and gait abnormalities which frequently occur in different combinations. The reported precipitating factors for developing FND following COVID-19 vaccination in individuals with biological social and/or psychological predispositions are primarily attributed to increased physiological awareness arousal and emotional processing [64]-[71]. Various studies have suggested that sensory connections are associated with atypical expectations and beliefs. This is the mechanistic equation for FND. COVID- 19 vaccination has resulted in only occasional case reports of Functional Neurological Disorder (FND) [72]-[77].
Globally numerous instances of primary and secondary orofacial neurological manifestations in COVID-19 were documented. Nevertheless, very few investigations determine the direct correlation between symptoms and the viral etiology. Investigating the impact and potential causal role of SARS-CoV-2 infection and associated vaccines is imperative. Future research should also assess the epidemiology of neurological manifestations clinical appearance and radiological findings. A more profound understanding would improve the preparedness of oral physicians to enhance the screening process ensuring that the Ministry of Health and Family Welfare receives accurate diagnoses appropriate management and concise reporting.
Ethical Approval: Institutional Review Board approval was not required.
Declaration of Patient Consent: Patient consent was not required as there are no patients in this study.
Financial Support and Sponsorship: Nil
Conflicts of Interest: The authors declare that they have no conflicts of interest.
Use of Artificial Intelligence (AI) - Assisted Technology for Manuscript Preparation: The authors confirm that no artificial intelligence (AI)- assisted technology was used to assist in the writing or editing of the manuscript, and no images were manipulated using AI tools.
AUTHOR CONTRIBUTIONS:
Manisha Lakhanpal Sharma: Conceptualized the study, developed the research design, and oversaw the overall project. He was responsible for data analysis and interpretation, as well as drafting the manuscript.
Simran Kaur: Assisted in the design and implementation of the study. Contributed to the development of the survey instrument, data collection, and analysis. Provided critical revisions to the manuscript.