Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-06-10
Accepted: 2025-08-22
Published: 2025-10-01
Pages: 204-209
Introduction: In forensic odontology, age determination of living individuals as part of establishing identity is becoming increasingly crucial. Several studies suggest that assessing the morphological features of adult human teeth using orthopantomograms is more dependable than other approaches for estimating age. These studies require that some corrections be made for size variations in the magnification of radiographs and angulations between the X-ray beam and film. To overcome this problem, some researchers suggest using the pulp/tooth area ratio instead of their direct measurement.
Methodology: This study describes an orthopantogram-based method for the estimation of age in living individuals from single-rooted premolars. The reliability of this method was cross-checked by taking measurements from the same sectioned teeth.
Result: We found that the radiographs were able to predict the age with 70% accuracy, and the tooth sections were able to predict the age with 73% accuracy. As there was a strong correlation of 85% between the two methods, they are similar in predicting the age of an individual.
Conclusion: We concluded that the radiographic method using orthopantomograms is a dependable non-invasive method for the estimation of age in living adult individuals.
Age is an important aspect in determining an individual's identity [1]. The need for age estimation in Forensic odontology in living individuals for establishing identity is becoming increasingly important, such as in scenarios where there are missing or uncertain birth data, for determination of minority or majority of age, and in the case of immigrants arriving in a country without sufficient identity documents [2],[3],[4] Most dental age estimation procedures necessitate the extraction and microscopic section preparation of at least one tooth. As a result, these invasive and destructive techniques are unsuitable for being employed on living individuals [5]. It may also be forbidden in the case of a dead person for several cultural and legal reasons. Moreover, tooth processing has the additional drawback of requiring the destruction of dental evidence. Hence, there is a need for non-invasive methods such as the use of radiographs. Radiographic examination is free of these drawbacks and can be regarded as a simpler, safer, and non-destructive approach [6]. One of the alternative approaches is the adoption of digitalized radiographs. These techniques employ image analysis to obtain non-destructive tooth measurements, which can be utilized for age determination [7]. Dental age determination using radiographs in children is based on tooth development phases. In adults, the continual life-long secondary dentin deposition as reflected by pulp area reduction is utilized [8]. Several studies have shown that OPGs are a reliable tool for age estimation [9]. However, some adjustments must be made to account for individual variability in tooth sizes, variations in radiograph magnification, and angulations between the x-ray beam and the film. To address this issue, some researchers propose employing the ratio of pulp and tooth surface areas rather than direct measurements [10]. This study elaborates on a method for age estimation of living adults from single-rooted premolars using orthopantomograms (OPG). The reliability of the radiographic method is verified by taking measurements of sectioned premolar teeth from the same individual following the OPG. This is an effort to establish the accuracy of the radiographic method.
The study was conducted at a dental college and hospital in Karnataka, India, and had a retrospective design with 30 individuals as the sample size. Two methods of age estimation using single-rooted premolars, namely the radiographic method and the tooth section method, were compared. Single-rooted premolar teeth from either jaw that were extracted for orthodontic purposes or due to poor periodontal prognosis were included. Data from 30 individuals (15 males and 15 females), where both the OPGs and extracted intact, single-rooted premolar teeth of the same individual were available, were included in the study. The other inclusion criterion was that the tooth was fully erupted with a completely formed root. Premolars with any pathologic conditions, such as periapical lesions, caries, which would modify the tooth surface area, mal-aligned or rotated premolars that affect the radiographic image, and premolars with restorations were excluded. The patient's chronological age was estimated by deducting the radiograph date from the patient's birth date. The study subjects’ age ranged from 13 to 70 years, with a mean of 34 years. For the radiographic method, the selected OPGs were digitalized using an X-ray scanner (Astra 4000 U) and the images were documented in a computer. For the tooth section method, the midline of the teeth was marked, sectioned mesio-distally, and photographed. The images of the radiographs and the sectioned teeth were uploaded into an image processing software (ImagePro Express version 4.0). From these images, the tooth and the pulp outlines were marked Figure 1 to obtain the surface areas of the tooth and the pulp, respectively. The tooth surface areas were divided by the pulp surface areas to obtain the pulp-to-tooth area ratios for each individual.

The values obtained were entered into a Microsoft Excel spreadsheet. The correlation coefficient was evaluated between the pulp/tooth surface area and age. Regression analysis was employed to compare the actual age and estimated age in both methods. A multiple linear regression model for age estimation was developed. Table 1 The regression equation explains the change in age when there is a unit change in the values obtained by the image.
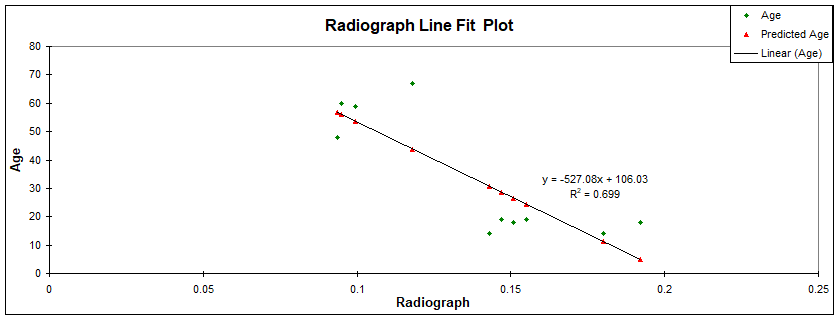
The estimated age was arrived at in both methods by using the surface area ratios of the pulp and tooth in the regression equation. On testing for the level of significance, both methods had a significant influence on age estimation (P<0.05%). The correlation coefficient between the estimated age and the chronological age in the radiographic method was 0.699, and in the tooth section method was 0.725, which demonstrated the linear relationship between the two variables Table 2, Figure 2 and Figure 3.
Hence, the radiographic method and tooth section method could predict the age with 69.9% and 72.5% accuracy, respectively. A correlation value of 0.85 was obtained, suggesting a strong correlation of 85% between radiographic and tooth section methods Table 3.
As there is a strong correlation between the two methods, they are similar in predicting age. We did not find any significant difference in morphological characteristics between the sexes, indicating that sex did not affect the regression model used for chronological age determination.
| Method | Regression equation |
|---|---|
| Radiographic method | Estimated Age = 106 - 527 x P/ T area ratio |
| Tooth section method | Estimated Age = 103 - 570 x P/ T area ratio |
| Predictor | Co-eff | SE Co-eff | R2 | P-Value |
|---|---|---|---|---|
| Radiographic method | -527.1 | 122.3 | 0.699 | 0.003 |
| Tooth Section method | -569.9 | 123.9 | 0.725 | 0.002 |
| Correlation | Radiographic method | Tooth Section method |
|---|---|---|
| Radiographic method | 1 | |
| Tooth section method | 0.85 | 1 |
Radiographic Method presents the relationship between estimated age and chronological age using the Radiographic method of age estimation. This method relies on the analysis of dental x-rays to assess the development and wear patterns of teeth, which can be correlated with age. The scatter plot displays the chronological age on the x-axis and the estimated age derived from radiographic data on the y-axis. Ideally, the data points should align along a diagonal line, suggesting a strong correlation between the actual age and the estimated age. A close alignment of the points to this line would indicate that the radiographic method is accurate in estimating chronological age. If the points deviate from the line, it suggests discrepancies in the method’s estimation, where the radiographic analysis may either overestimate or underestimate the age.
Tooth Section Method shows a similar plot, but for the Tooth section method, which involves the examination of the internal structure of teeth, such as the size of the pulp chamber and dentin layers, after the teeth are sectioned. This method provides a microscopic approach to age estimation. The scatter plot in this case also uses chronological age on the x-axis and estimated age on the y-axis. A strong correlation between the two variables would again be represented by points closely aligning along a diagonal line. Deviation from this ideal line may indicate inconsistencies in the method's predictions, suggesting that it could either overestimate or underestimate an individual's age.
Comparing the two plots, one can evaluate the accuracy of the Radiographic method versus the Tooth section method. If the points in Figure 2 (Radiographic method) are more tightly grouped along the diagonal line, it would indicate that the radiographic method is more reliable in estimating chronological age. However, if the points in Figure 3 (Tooth section method) show a closer alignment to the diagonal, the Tooth section method may be considered more precise. These scatter plots provide essential visual insights into the performance of both methods, highlighting their strengths and potential limitations, which could guide further refinement of age estimation techniques.


The age estimation of living adults is a critical aspect of forensic odontology, especially in circumstances requiring the establishment of identity for legal and social purposes. The present study aimed to evaluate the reliability of using pulp to tooth area ratios derived from OPGs for age estimation and to compare these findings with direct measurements from sectioned teeth.
Our findings demonstrate that the pulp-to-tooth area ratio obtained from radiographs predicted age with 70% accuracy, which is comparable to the 73% accuracy from sectioned teeth, and the strong correlation (r = 0.85) suggests both methods are closely aligned in their predictive capability. These findings are consistent with previous studies that have validated the use of pulp size reduction as a marker for age estimation.
Cameriere et al [7], founded the pulp-to-tooth area ratios analysis using periapical radiographs of single-rooted teeth and reported high correlations between reduced pulp size due to secondary dentin deposition and chronological age. Similar findings have been obtained by Kvaal et al [2]. who developed a method using pulp to tooth ratios on different teeth from OPGs and intraoral radiographs. Their method accounted for magnification errors by utilizing ratios rather than direct measurements, a technique also adopted in our study to overcome variations in radiographic angulation and magnification.
The deposition of secondary dentin, a lifelong process, diminishes the size of the pulp chamber and is well established as a valid biological marker for ageing [10]. Population-specific variations in secondary dentin deposition have been documented, underscoring the importance of developing regression models specific to regional populations [11]. Factors, such as dental pathologies and restorations, can affect pulp size and should be considered when interpreting results; hence, our study excluded teeth with evident abnormalities to minimize these confounding variables.
Most of the dental age estimation methods necessitate teeth extraction, and some of them need at least one tooth section preparation for microscopic examination. These procedures take time, and a damaging approach may not be appropriate for ethical, religious, cultural, or scientific reasons [2]. Hence, there is a need for non-invasive dental imaging techniques, especially in living individuals. Advanced imaging techniques such as cone-beam computer tomography (CBCT) have become available in recent times, which offer a three- dimensional view. Many studies on CBCT dental age estimation using pulp-to-tooth volume ratios among various populations have shown good results [12],[13],[14],[15]. However, dental OPGs were considered in our study as they are cost-effective and widely employed. OPG radiographs have an innate disadvantage of image distortion due to the two-dimensional projection of the curved dental arches [9]. Hence, the current study intended to establish the accuracy of the dental age estimation using panoramic radiography by using the pulp-to- tooth area ratio of a single-rooted premolar tooth and comparing it with standardized photographs of the same sectioned tooth.
Maxillary canines are the preferred teeth for dental age estimation as they have a single root and the largest pulp area. In addition, they are quite strong, suffer less attrition in comparison to other posterior teeth, and they usually endure even in older individuals [10],[16],[17]. Premolars from both arches were chosen in the current study due to the ease of availability of extracted intact premolars, which are commonly extracted for orthodontic purposes and in patients with poor periodontal prognosis.
Also, only single-rooted premolars were considered to eliminate the superimposition of root images on the radiograph, which is often encountered in multirooted teeth. Our results have shown that single-rooted premolars from either jaw can be used for age estimation.
Our results did not find significant differences in morphological characteristics between the genders, indicating that gender did not affect the regression model used for estimating chronological age using pulp/ tooth area ratios. Despite the positive results obtained from our study, we observed that this approach of estimating age had a few limitations. This method cannot be applied in multirooted teeth, as obtaining precise dimensions is difficult due to the superimposition of root images in the radiographs. The expense of installing the software is also significant. The values are subjected to intra- & inter- examiner variations. Since our sample size was small, further large-scale studies are required using different teeth to establish the radiographic method as a standard protocol for age estimation. Future studies should explore incorporating machine learning algorithms to enhance accuracy and automate measurements.
This study demonstrates that the non-invasive and convenient method of recording the pulp/tooth area ratio of single-rooted premolar teeth derived from orthopantomograms can be dependably employed in the chronological age estimation of an adult living individual. However, for forensic applications, the method should be validated across diverse populations and larger sample sizes to establish its robustness and legal admissibility.