Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-06-01
Accepted: 2025-08-27
Published: 2025-01-10
Pages: 217-223
Background: Traumatic injuries to anterior teeth often result in pulpal necrosis and incomplete root development, posing challenges for both endodontic and esthetic rehabilitation. Traditional apexification methods have evolved with the advent of bioceramic materials, which now allow for more predictable outcomes. In addition, patient esthetic expectations necessitate an integrated approach combining both restorative and cosmetic procedures.
Case Presentation: A 20-year-old female presented with a discoloured and previously traumatized maxillary right central incisor (#11), which had undergone failed root canal treatment and exhibited an open apex. Clinical and radiographic examinations revealed periapical pathology and an inadequately obturated canal. Nonsurgical endodontic retreatment was initiated, followed by apexification using MTA to establish an apical barrier and BIO-C repair for complete Bio-obturation. Subsequent internal bleaching was performed to address intrinsic discoloration, and the final esthetic outcome was achieved with an indirect composite veneer. Follow-up visits confirmed resolution of periapical pathology and satisfactory esthetics and function.
Conclusion: This case demonstrates that a stepwise, minimally invasive approach involving endodontic retreatment along with bioactive material-based apexification, internal bleaching, and conservative restorative techniques can successfully manage complex cases involving open apices and anterior tooth discoloration. The preservation of natural tooth structure and restoration of esthetics are achievable with careful planning and execution.
Traumatic dental injuries present a global clinical challenge, often resulting in damage not only to the tooth and neurovascular supply of the pulp but also to the surrounding periodontal structures and alveolar bone. These injuries represent approximately 5% of all dental consultations and are particularly concerning when they involve immature permanent teeth. One of the most serious consequences of trauma in such cases is pulp necrosis, which halts further root development. This leads to the formation of thin dentinal walls and open apices, making the tooth structurally weak and complicating effective root canal debridement and sealing [1]. Historically, apexification has been the preferred treatment modality for managing immature teeth. The conventional method used calcium hydroxide to promote apical barrier formation over time. Yet, this technique requires multiple appointments over several months, posing challenges in terms of patient compliance and follow-up [2]. Additionally, prolonged exposure to calcium hydroxide can compromise the integrity of the root dentin, increasing the risk of fracture [3]. In response to these limitations, mineral trioxide aggregate (MTA), a calcium silicate-based cement introduced by Torabinejad et al., became widely adopted in endodontics [4].
MTA demonstrated excellent biocompatibility, antibacterial properties, low solubility, and the ability to expand slightly upon setting making it ideal for creating an artificial apical plug [5]. Regenerative endodontic procedures (REPs) have also evolved as an innovative approach for treating necrotic immature teeth. First conceptualized by Nygaard-Østby in 1961, these biologically based treatments aim to regenerate dentin, root structures, and the pulp–dentin complex. Typically performed in two appointments, the first involves disinfection and placement of intracanal medicaments, followed by induction of bleeding into the canal space in the second visit. MTA is then placed over the blood clot, and the tooth is sealed coronally. While promising, REPs have shown variability in outcomes particularly in achieving consistent root maturation and apical closure [6]. Apexification, in contrast, remains a reliable and predictable method, with several studies confirming its success in resolving periapical pathology, achieving apical barrier formation, and promoting radiographic closure. Histological analyses have shown the development of mineralized tissues such as cementum-like, bone-like, or osteodentin-like structures at the apex following apexification [7].
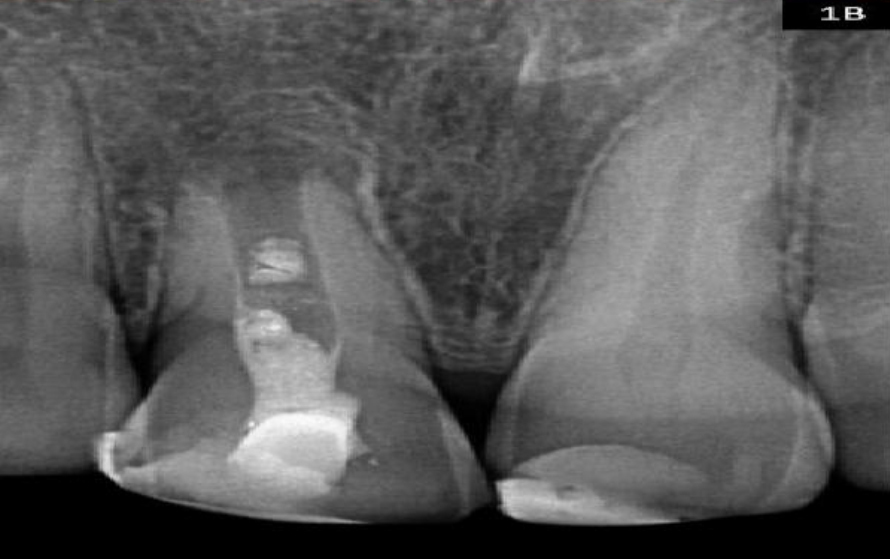
A 24-year-old female presented to the Department of Conservative Dentistry and Endodontics, KLE VK Institute of Dental Sciences, complaining of mild to moderate pain on biting, intermittent pus discharge, and discoloration of her upper front tooth over the past six months. She reported dental trauma approximately five years ago, followed by root canal treatment at a private clinic. Her medical history was non-contributory. Intraoral examination revealed a defective tooth-coloured restoration and mild crown discoloration with #11 and a previous discoloured restoration with #21. Pulp testing with Endo-Frost (Coltène, Langenau, Germany) and an electric pulp tester (Parkell Electric tester, Redmond, USA), revealed no response with #11, and immediate response with 2#1. Tooth #11 was tender on percussion and palpation, while #21 was non-tender. Both teeth showed probing depths were within normal limits and no mobility. The pre-operative radiograph showed an underextended root canal filling, terminating short of the apex. The apical portion of the root displayed a blunderbuss canal configuration with an open apex and shortened root length. Based on the clinical and radiographic evaluation, the tooth was diagnosed as previously treated, with a failed regenerative endodontic procedure and symptomatic apical abscess. The available endodontic treatment options, including nonsurgical root canal retreatment, were thoroughly discussed with the patient prior to initiating treatment with either regenerative endodontic treatment (RET), or one-step apexification using MTA. One step apexification was chosen as the treatment option. Additionally, the patient requested esthetic improvement, for which internal bleaching and indirect veneer restoration were planned after completion of the endodontic phase.
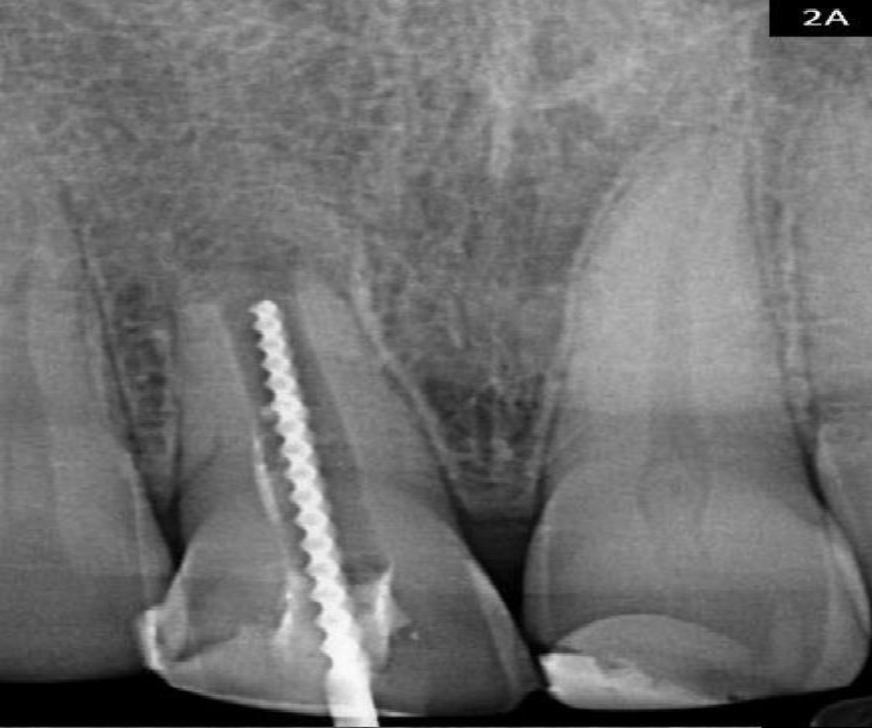
First visit: Following administration of local anesthesia (2% lignocaine with 1:80,000 epinephrine), the tooth was isolated under a rubber dam to ensure an aseptic working field. Under magnification with an operating microscope (ZEISS Microscopy, Germany), the previous composite restoration was removed, and the access cavity was re-entered. The existing MTA material was removed using ultrasonic tips. Working length was established using an apex locator (Root ZX, J. Morita, Japan), which was confirmed radiographically. Figure 2A The canal was not mechanically enlarged to preserve the already thin dentinal walls. Irrigation was done using 3% sodium hypochlorite (NaOCl), followed by a final rinse with sterile saline. The canal was dried with paper points, and calcium hydroxide paste (Calcipex II, Japan) was placed as an intracanal medicament. Figure 2B The access was sealed with Cavit G (3M ESPE, Germany).
Second Visit: The patient was asymptomatic, and the sinus tract had resolved. After local anesthesia and rubber dam isolation, the calcium hydroxide dressing was removed. The canal was irrigated thoroughly with 3% NaOCl (Vishal Dentocare, Ahmedabad) and flushed with saline. After drying the canal with paper points, a 5 mm apical plug of MTA (ANGELUS®, Brazil) was placed and condensed using hand pluggers (GDC, India). A radiograph was taken to verify the plug position. Once the MTA plug was set, the remaining canal was filled with BIO-C® REPAIR (Angelus, Brazil), a bioactive material with sealing and biocompatibility properties. A radiograph confirmed adequate obturation. Figure 2C
Third Visit: Upon confirming the absence of symptoms and a complete set of the MTA, the access cavity was cleaned and restored with a 1–2 mm base of glass ionomer cement (Ketac™ Molar, 3M ESPE) to seal the canal coronally. Internal bleaching was initiated using a paste of 3% sodium perborate and distilled water (3:1 ratio). The cavity was sealed with temporary restorative material. The patient was recalled weekly for shade evaluation and repeated bleaching. The shade was monitored using the VITA classical shade guide and standardized clinical photographs. After three applications, a significant improvement in tooth shade was observed. The cavity was sealed permanently using a light-cured composite Filtek™ Z350 XT (3M Seefeld, Germany). Figure 3A Fourth Visit: After 2 weeks, patient was recalled and the tooth surface was prepared for the indirect veneer with #11 and #21. Figure 3B A digital impression was recorded using an intraoral scanner (Dentsply Sirona CEREC Primescan, North Carolina, USA). Temporization was done using OraTemp (Prevest DenPro Ltd, Jammu) The veneers were fabricated by the lab. Figure 4A, 4B
Final Visit: The fit and esthetics of the veneers were verified intraorally. After rubber dam isolation, adhesive bonding was performed. Final finishing and polishing were carried out, and occlusion was adjusted to avoid premature contacts.








Traumatic injuries to immature permanent teeth frequently lead to pulpal inflammation or necrosis, disrupting normal root development and resulting in thin dentinal walls and open apices. These anatomical challenges complicate the establishment of an adequate apical barrier and a three-dimensional seal during endodontic treatment. The management of such teeth becomes increasingly complex in the presence of an associated periapical infection, which further compromises the healing potential and treatment outcomes. [8]. Endodontic management of such teeth typically involves either conventional apexification techniques or regenerative approaches such as revascularization. Pulp revascularization is a favourable treatment option in these cases, offering the potential for continued root development and reinforcement of dentinal walls; however, its applicability is generally confined to patients between 8 and 16 years of age. Considering the prior failure of revascularization, apexification was chosen as the preferred treatment option. The primary objective of apexification is to create a mineralized apical barrier, which serves to prevent the infiltration of toxins and bacteria into the periapical tissues from the root canal. Additionally, this barrier is essential for ensuring effective compaction of the root-filling material [8]. Several hypotheses have been proposed to explain the failure of regenerative endodontic procedures (REPs). One possible factor is the persistence of bacteria in the apical region of the root canal. Another is the dislodgement or inadequate formation of the blood clot, potentially leading to voids within the canal space. Furthermore, failure to establish a proper coronal seal may also compromise the treatment success [9]. Calcium hydroxide has traditionally been employed for apexification. Still, its use is associated with several limitations, including the extended duration required for apical barrier formation, which often ranges between 5 to 20 months, reducing patient compliance, risk of reinfection due to loss of temporary restorations between visits, and a potential reduction in the fracture resistance of the treated tooth [8]. Mineral trioxide aggregate (MTA) is a preferred material for apexification due to its superior biocompatibility, bioactivity and sealing ability. Its high pH (~12.5) provides antimicrobial action and bioinductive properties that promote cementum formation and periapical healing. MTA forms a tight apical barrier by bonding to dentinal walls, creating a monoblock effect, minimizing microleakage. Additionally, fast-setting variants reduce the number of required clinical visits, enhancing treatment efficiency [9]. In addition to its biocompatibility, antimicrobial properties, and ability to prevent marginal infiltration, mineral trioxide aggregate (MTA) offers superior resistance to coronal microleakage. It reduces the risk of tooth fracture compared to calcium hydroxide [10]. Besides the challenge posed by the open apex, managing the associated chronic periapical lesion also required careful consideration. Irrigation with sodium hypochlorite alone may not achieve complete disinfection of the root canal system. Residual bacteria that survive instrumentation can multiply during the interval between appointments, potentially recolonizing the canal space. Consequently, calcium hydroxide was employed as an intracanal medicament between appointments to eradicate microorganisms. Its antimicrobial efficacy is due to the dissociation into calcium and hydroxyl ions, creating a highly alkaline environment that disrupts enzymatic functions vital for bacterial survival, metabolism, growth, and replication [8]. Pawan Darak et al. reported that the teeth with the entire canal obturated using MTA exhibited the highest fracture resistance, followed by those filled with Biodentine. This enhanced reinforcement is attributed to the bioactive properties of both materials, which promote the formation of a hydroxyapatite layer at the dentin–material interface, thereby improving the structural integrity of the root. Our findings align with those of Milani et al., who suggested that the modulus of elasticity between MTA and dentin is comparable and likely the primary factor contributing to MTA’s reinforcing effect [11]. Another contributing factor could be the inability of gutta-percha to strengthen the compromised cervical region of the root, which may explain the lower resistance to fracture observed in groups with an apical plug. This limitation is attributed to gutta-percha's poor cohesive strength and low modulus of elasticity [9]. Consequently, bio-obturation with materials like MTA presents a more viable option for enhancing root strength. Tooth discoloration is a common side effect following regenerative endodontic procedures (REP) or MTA apexification. This is primarily attributed to the presence of bismuth oxide, a radiopacifier commonly used in MTA formulations [12]. Kênia Soares de Toubes et al. reported that Bio-C Repair results in significantly less discoloration compared to MTA, mainly due to its non-staining formulation with zirconium oxide [13]. In our study, to minimize the risk of discoloration, we placed a 3 mm layer of Bio-C Repair over the apical plug with MTA. Due to discoloration resulting from the previous endodontic treatment, non-vital bleaching was initially performed to improve the tooth’s esthetics. After achieving satisfactory lightening over two sessions, a more definitive and long-term esthetic solution was chosen in the form of indirect lithium disilicate (Emax) veneers. These restorations offer superior optical properties, including excellent translucency and light transmission, which closely replicate the natural enamel. Their ability to mimic the luster and depth of real teeth makes them an ideal choice for achieving a bright, harmonious smile with long-lasting esthetic results [14].
This case highlights the multidisciplinary management of a previously traumatized and endodontically failed maxillary central incisor with an open apex. Through a combination of nonsurgical endodontic retreatment, apexification with Biodentine, internal bleaching, and indirect composite veneer placement, functional and esthetic rehabilitation was successfully achieved. The outcome underscores the importance of preserving natural dentition and demonstrates how conservative approaches, when applied sequentially and appropriately, can yield favourable long-term results in complex cases.
I had been apprehensive about the discoloration of my front tooth from the trauma of the earlier events. My root canal treatment from before was unsuccessful, as the tooth was beginning to discolor and hurt. On my visit to the clinic, the dentist explained diplomatically that the tooth had an open apex, and that the standard treatment for my case would not work. Hearing about the newer, minimally invasive treatment was a huge relief. MTA and other bioactive materials would help with the restoration of the function and appearance. Over the course of treatment, I had to make multiple visits to the clinic. Although I was a bit nervous, the dentist eased my worries, and with the help of local anesthesia, I felt no pain. MTA was used to fill the canal and also help with the internal bleaching process to help improve the color of the tooth. After a couple of weeks, the last step was done, and the dentist placed the veneer. I was happy with my smile. I was also happy that my tooth was now functioning and felt so strong. I am really pleased with the results and how the dentist's care and expertise helped return my confidence. The procedure was easier than I thought and I am thankful for how the staff helped with my smiling restoration.
