Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-06-15
Accepted: 2025-09-25
Published: 2025-10-01
Pages: 224-232
Background: A common occurrence in endodontic treatment, root canal perforation (RCP) originates from the accidental connection between the periodontal space and the root canal. Among the various issues this condition can bring about are tooth loss, periapical lesions, and infection. Correct outcomes depend on proper treatment and early diagnosis.
Case Presentation: Forty-year-old patient presented with mild discomfort, some dental movement, and greyish discoloration of tooth number 11. Clinical and radiographic exams found gutta-percha expelled from a root canal hole. A cone beam computed tomography (CBCT) scan was used to assess the size, position, degree of the hole, and concomitant periapical illness. Bone grafting and simultaneously apical sealing were used in the surgical intervention using Mineral Trioxide Aggregate (MTA) for obturation.
Six months later follow-up showed significant with growth of new bone. CBCT imaging is necessary for RCP's correct diagnosis and surgical planning, to ensure accurate intervention. MTA sealed the hole tightly, also accelerating healing and preventing further infection. This case demonstrates how well-advanced imaging mixed with biocompatible materials performs to have favorable outcomes in challenging endodontic treatments.
Conclusion: MTA obturation and CBCT imaging are therefore valuable tools in the management of root canal perforations, improving diagnostic accuracy, treatment precision, and long-term healing, and so patient outcomes.
Root canal perforation (RCP) is a clinical condition caused by an unintentional connection between the periodontal space and the crown or root canals [1]. Many times, errors during endodontic treatments such as incorrect instrumentation or excessively vigorous attempts to clean the root canal system cause this condition [2]. Among the main problems RCP might bring about are dental loss of function, constant infection, and periapical diseases. The prognosis for teeth with root canal perforations is affected by the degree of the periapical illness, the size, and location of the hole, the time passed since the perforation occurred, and the kind of treatment received [3].
Root canal perforations have traditionally been difficult to find and treat under limited imaging capabilities. Cone Beam Computed Tomography (CBCT) has changed the field of endodontics with an extremely comprehensive, three-dimensional imaging of the root canal system, surrounding bone, and other anatomical components [4]. CBCT imaging not only helps clinicians exactly pinpoint, the location, and extent of perforations but also any concomitant periapical tumors, cysts, or other disorders. This degree of precision in diagnosis assists clinicians to make more smart choices regarding treatment course and prognosis, therefore improving the chances of beneficial results [5].
In the present case report using a surgical approach, root canal perforation was under control; CBCT is an essential diagnostic tool. The imaging allowed one to completely evaluate the position of the hole and the surrounding structures, thereby ensuring that the most appropriate treatment plan was devised. The clinical and radiological findings guided one to choose the root canal obturating agent to be Mineral Trioxide Aggregate (MTA). MTA, a biocompatible material, has become very well-known in endodontic treatment thanks to its remarkable sealing properties, capacity to promote healing of periapical tissues, and resistance to occlusion forces [6].
MTA has shown very great efficacy in reducing root canal perforations, especially in cases of major periapical disease. Excellent material sealing capability helps to prevent bacterial access into the root canal system, therefore reducing the infection risk [7].
MTA also aids in the development of hard tissue barriers, therefore enabling the surrounding soft tissue and bone healing. MTA's properties make it especially suitable for challenging endodontic cases where traditional filler materials and sealers may not be sufficient [8]. MTA may help patients with noteworthy periapical lesions or inflammation to have a more positive outcome thereby preserving the tooth and its function [9].
Moreover, the CBCT imaging applied in this case ensured that the surgical approach was correct and least invasive. The three- dimensional perspective of CBCT enabled the practitioner to apply the therapy with better accuracy and helped to avoid unnecessary damage to surrounding structures [10]. This case highlights the effectiveness of a modern, integrated approach to address challenging endodontic problems by combining CBCT's enhanced diagnostic skills with MTA's therapeutic benefits.
All things considered, root canal perforation is a main issue requiring careful inspection and treatment. Cone Beam Computed Tomography has substantially enhanced our ability to detect and treat such disorders by the use of thorough, three-dimensional imaging [11],[12]. CBCT coupled with MTA obturation achieved an acceptable treatment outcome in the present context, therefore demonstrating MTA is an excellent material for treating root canal perforations especially in cases when traditional procedures would not be enough. This case illustrates the importance of employing biocompatible materials and advanced diagnostic instruments in modern endodontics to attain optimum results and improve patient outcomes [13].
On Extra-oral examination, no facial asymmetry was noted, the lip was potentially competent and there were no tender or palpable lymph nodes detected upon palpation Figure 1. Upon clinical examination, a grayish discoloration and slight mobility were observed w.r.t 11 and 21 Figure 2.


Table 1 shows a thorough study of tooth number 11 together with the findings of many diagnostic procedures used to evaluate its condition. The mildly to moderately uncomfortable palpation and percussion tests point to possible inflammation or sensitivity in the nearby tissues. With a mobility score of 2, the probing measurements (MD BL) and mobility test show typical results—that is, minor tooth movement but still within reasonable bounds. While the heat and electric pulp tests (EPT) showed no reaction, maybe indicating a lack of nerve sensitivity or necrosis within the tooth, the transillumination test revealed no fractures or fissures. Furthermore, noted by the anesthetic test and discoloration observation was a greyish discoloration that could point to an underlying injury or damaged tooth structure. These results together suggest a possibly compromised tooth that could call for more research or treatment.
At the middle third of the root canal and gutta-percha extruding out of the root canal, the pictures revealed an interruption and little displacement of the filling material Figure 3. To thus enhance the localization of and access to the RCP, a Cone Beam Computed Tomography was acquired. An RCP was seen in the middle third of the buccal surface in the sagittal plane with more than 6mm of gutta- percha cone extrudes pointing forward from the root canal Figure 4.
Coronal Structure: Hyperdensity observed with coronal aspect extending into radicular pulp is suggestive of an endodontically treated tooth Root and root canal: A single canal is seen which is slightly curved distally at the apical third level. Evidence of restoration beyond the apex on the labial aspect at the middle third level is suggestive of suspected perforation Figure 4.
Hypodensity observed within radicular pulp is suggestive of internal resorption. Canal Length – 22.7mm (from the incisal edge to the apex) Periapical Region: Hypodensity observed at the periapex of the tooth with a breach in the labial bone plate extending distally up to the mesial aspect of periapex of 12 is suggestive of periapical pathology/scar Figure 5. Periodontal Region: Evidence of mild periodontal bone loss was observed on mesial & distal aspects.
Table 2 offers a thorough radiographic study of tooth number 11, which has had root canal therapy. It shows that the tooth has an oval- shaped single root canal free of anatomical variances. The apical third stays uninstrumented during the treatment; the apex of the root is closed. The absence of calcification within the canal suggests that hard tissue does not restrict or block the canal. Still, both internal and external resorption point to continuous structural deterioration of the tooth. These results draw attention to the treatment history of the tooth and point to any issues that could call for additional examination or intervention.
Table 3 shows in addition to a fracture evaluation and radiographic diagnostic the periodontal, periapical, and endodontic state of tooth number 11. The loss of lamina dura points to probable periodontal issues around the tooth; yet, the remaining crestal bone implies no appreciable bone loss. Observation of the widening of the periodontal ligament (PDL) suggests either inflammation or another pathogenic state. Notable also is periapical radiolucency (PA RL), which points to probable injury or infection at the root apex.
Root canal therapy has a recorded history for this tooth; during this process, a hole in the middle third of the buccal surface of the root canal was found. An insufficient or partial root filling is indicated by a 6mm section of gutta- percha emerging from the root canal. No retrograde filling is seen. During the fracture evaluation, no fractures were found in the crown, root, or any part of the tooth. Further evaluation by cone beam computed tomography (CBCT) is indicated to determine the degree of the damage and guide treatment options. The radiographic diagnostic shows a root canal rupture connected with a periapical lesion.
Table 4 shows, based on radiographic results and clinical examination, the final diagnosis and treatment plan for tooth number 11. To completely appreciate the degree of the damage, one must take into account the differential diagnosis including root canal perforation linked with certain periapical disorders, such as periapical cyst, periapical scar, periapical granuloma, and periapical abscess.
Following extensive cone beam computed tomography (CBCT) analysis helped to clarify the prognosis and possible therapy results, therefore guiding the development of the treatment strategy. A surgical technique was advised considering the intricacy of the case as the traditional approach would probably have damaged the tooth much more. The treatment plan addresses the hole and stops further damage by including simultaneous apical sealing and mineral trioxide aggregate (MTA) obturation of the canal. The tooth's long-term efficacy of the therapy and general condition of the tooth are under doubt, hence the prognosis for the tooth is seen as dubious.
A trapezoidal full-thickness mucoperiosteal flap was raised using no. 15 blades under buccal local infiltration and nasopalatine nerve block. The osteotomy site was evaluated and produced to locate the root end. Periapical curettage was carried out using no. 1 and 2 Gracey curetts to remove the granulation tissue. The tissue was sent for Biopsy and the final diagnosis resulted in a Periapical Cyst. The infected GP point was removed, the weakened root was resected and the root end was recontoured Canal was irrigated well with saline.; retrograde irrigation of canal space was done with full strength NaOcl (3%) with simultaneous suction from coronal access followed by obturation of canal with ProRoot MTA(Dentsply) mixed with 0.12% chlorhexidine Conventional compaction was carried out using finger pluggers. Finally, a bone allograft (0.5cc) (from Novabone) and bone xenograft (from osseograft) were mixed place.
A collagen membrane was over the surgical window to accelerate bone regeneration and the flap was repositioned, followed by interrupted sutures with 3-0 silk thread. Postoperative periapical radiography was performed immediately after suturing. The sutures were removed after ten days, and the patient progressed well postoperatively without intercurrences Figure 6.
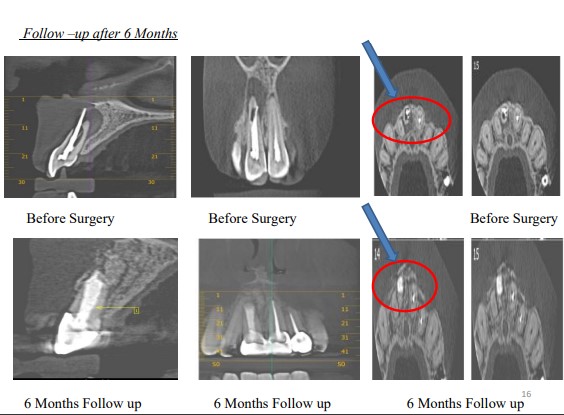
Following thirty days and six months, two follow-up sessions were conducted; the patient is recalled for additional examination for nine months, one year, and two years. These sessions included radiographic and clinical intraoral examinations in addition. The patient is symptom-free; the periapical lesion has started to mend; and new bone is visible. Six months later, the patient's development was assessed using CBCT images, and a bone neoformation was noted at tooth number 11's periapical region. Figure 7,8.



| Tooth Number | Palpation (WNL) | Percussion (WNL) | Mobility (1-4) | Transillumination to assess the fracture | Thermal Tests | EPT WNL Hyper Response | Probing | Other Test |
|---|---|---|---|---|---|---|---|---|
| 11 | ++ | ++ | 2 | nil | No Response | Nil | 2333 | Grayish Discoloration |
| Tooth Number | #11 |
|---|---|
| Caries involvement | Root Canal Treated |
| Nature of the root canal involved | |
| Number of canals | 1 |
| Shape | Oval |
| Anatomical variation | Nil |
| Closure of the apex | Closed apex (uninstrumented apical third) |
| Calcification | Nil |
| Resorption | Internal and Resorption evident |
| Periodontal and Periapical Status | |
| Lamina Dura | Lost |
| Crestal Bone Loss | Intact |
| Periodontal Ligament Widening | Present |
| PA Radiolucency (RL) | Present |
| Previous Endodontic Treatment | |
| Status of Root Canal Filling | Root Canal Perforation in middle third of Buccal Surface with 6mm Gutta Percha extruding out of root canal |
| Fracture Assessment | |
| Radiodiagnosis | Root Canal Perforation associated with periapical lesion. Cone Beam Computed Tomography was advised to the patient for further evaluation |
| DIAGNOSIS | |
|---|---|
| Diagnosis And Differential Diagnosis After proper CBCT analysis and calculation of prognosis and treatment outcome, surgical management was structured for this case Conventional approach would have further compromised the tooth, therefore simultaneous apical sealing and MTA obturation of the canal was planned | Differential Diagnosis: Root Canal Perforation associated with Periapical cyst Root Canal Perforation associated with Periapical scar Root Canal Perforation associated with Periapical granuloma Root Canal Perforation associated with Periapical abscess |
| Treatment plan with references | After proper CBCT analysis and calculation of prognosis and treatment outcome, surgical management was structured for this case Conventional approach would have further compromised the tooth , therefore simultaneous apical sealing and MTA obturation of the canal was planned |
| Prognosis | Questionable |



RCP is seen as a major operational mistake in surgery. A good prognosis is usually obtained if a limited, correctly diagnosed condition is sealed with biomaterial [14]. CBCT's application in diagnosis brought enhanced surgical planning of RCP, greater security, and proper placement. Following the three-dimensional picture vision improved the organization of the surgical management and planning. Emerging as a consistent bioactive material with wide uses in endodontics including the obturation of the root canal space is mineral trioxide aggregate (MTA) [15].
MTA is a bioactive silicate cement that not only irritates periapical tissues but also stimulates PDL and cementum renewal. '' When this osteoinductive and cementogenic material is utilized to fill the root canal system, failed root canal procedures hampered by microleakage, insufficient cleaning and shaping, poor quality obturations, and extensive periapical lesions show better healing rates. MTA-obturated teeth seem to not only improve their fracture resistance over time but also effectively entomb and neutralize germs in very infected teeth [16],[17].
Finally, by enabling exact localization and minimum invasive procedures, Cone Beam Computed Tomography (CBCT) greatly improves the diagnostic and treatment planning of root canal perforations. For closing holes and encouraging tissue healing, mineral trioxide aggregate (MTA) seems to be a biocompatible and useful substance. These cutting-edge methods taken together produce good results that preserve dental function and stop further issues. This instance emphasizes the vital part contemporary diagnostic tools and materials play in obtaining good endodontic treatment outcomes.
As an individual of 40 years of age, specifically with regards to tooth number 11, I had mild pain and issues with the mobility of the tooth. I also saw and became worried about the tooth starting to change color and appear grey. I later learned about the insidious issues after venturing to the dentist. It was after this visit that I learned that the issues were far more complicated and sinister than I had thought. The dentist stated that I had root canal perforation (RCP) and explained that this is a complication that happens when the root canal inadvertently communicates with the periodontal space.
I was unfortunately informed that this was also due to the root canal that I had previously. The dentist informed me that this was the beginning of a larger problem, then explained how the perforation was the cause of an infection and, without addressing it, the potential loss of the tooth. I was particularly distressed to find out that a piece of what is referred to as root canal filling material, gutta-percha, had been released from the root canal. It was due to the perforation and this explained the pain as well as the mobility of the tooth.
As the dentist explained to me, the best option to remedy the situation was to perform surgery to close the hole and stop the damage from getting worse. I was told that the more effective method to assess the damage was to use Cone Beam Computed Tomography (CBCT) imaging rather than traditional X-rays, which to my delight had been insufficient to assess the situation. The more detailed imaging obtained from the CBCT scan would offer the dentist a complete three-dimensional view of the tooth and the adjacent soft tissues, thereby allowing for more precise surgical planning.
The treatment plan involved the use of Mineral Trioxide Aggregate (MTA), which I was told would entail closing the hole and also, biocompatibly, would promote healing of the adjacent tissues. The dentist explained to me that this meant the material would seal the hole and also promote the recovery of the adjacent soft tissues and bone that had their integrity compromised by infection. Hearing this eased my worries about this tooth and its future.
I was required to receive a bone graft, which is a common procedure performed in dentistry, during my surgery. The dentist told me that the graft is necessary as it helps to regenerate the bone that is required in the region of the tooth in order to create support and minimize the chance of future complications. I understood that the procedure might be extensive, but considering the situation, I understood the risks of losing a tooth and the consequences that it may lead to, which made me realize that it had to be done.
I was quite nervous the day of the surgery, but I was also excited that the treatment would be able to fix the issue. To get to the problematic tooth, the dentist performed a full-thickness mucoperiosteal flap. The procedure was performed while I was under local anesthesia, which meant that I was not able to feel any pain during the surgery. After the surgery, I was told to adhere to a certain criterion of post-operative care which included taking the medications that were prescribed to me and attending the subsequent appointments that were made to keep track of my healing.
In the weeks that followed, the surgeries, I had three more AP appointments and all three gave me more and more confidence that everything was healing well. The extra sensitivity and mobility I had over the previous few weeks was starting to go away, and by the six month mark, things were looking pretty good. The various CBCT's showed casing the new bone that was developing around the tooth, a sign that I had been told was a big indication that the surgery was a success, and a sign that I was also symptom free was a big relief.
It is in retrospect that I am the most thankful for the CBCT and other various tools that I was able to have the services of a dentist who was able to identify exactly what was going wrong and for that made the treatment plan a combination of good and several lower was very effective duplicate. The MTA and the specialized bone grafting have helped preserve the tooth in the construction of good confidence that the tooth will function normally for a long time. As a result of the good treatment approach the dental health and tooth overall peace of mind have improved. Overall, the good treatment of saved the tooth from further issue, and I’m thankful for all the people who made the services of the good treatment.