Oral Sphere
Journal of Dental and Health Sciences
Journal of Dental and Health Sciences
Received: 2025-06-01
Accepted: 2025-12-26
Published: 2026-01-01
Pages: 36-40
Background: Successful endodontic treatment depends on comprehensive knowledge of root canal anatomy. However, complex canal configurations, especially in mandibular first molars, pose diagnostic and therapeutic challenges. One such anatomical variation is the middle mesial canal (mmc), situated between the mesiobuccal (mb) and mesiolingual (ml) canals. Often undetected in conventional radiographs due to its narrow, calcified nature, failure to identify and treat the MMC may result in persistent infection and treatment failure. Enhanced magnification and advanced diagnostic tools like CBCT and dental operating microscopes (dom) have improved the detection of such variations.
Case Presentation: A 26-year-old female presented with deep caries and tenderness in the mandibular left first molar (tooth #36). Clinical and radiographic examination confirmed pulpal necrosis with symptomatic apical periodontitis. Following informed consent and isolation, an access cavity was prepared. Under DOM, an additional canal orifice identified as an MMC was located between the MB and ML canals. Following this, working lengths were confirmed, instrumentation was done, and obturation and post-endodontic restoration were completed.
Conclusion: This case highlights the importance of careful access cavity preparation, the use of magnification, and ultrasonic instrumentation in detecting and managing middle mesial canals (MMCs). Modern endodontic tools such as the dental operating microscope and ultrasonic tips play a vital role in revealing these often-hidden anatomical variations, which are essential to clean and seal for long-term success. Missing such canals can compromise treatment outcomes. Therefore, clinicians should remain vigilant, especially when treating mandibular first molars, and take time to explore the pulpal floor for any additional canal openings thoroughly. Recognizing and addressing these variations early in treatment can significantly enhance the prognosis and longevity of endodontic therapy.
For endodontic therapy to be successful, it is essential to comprehend the anatomy of the root canal. Nonetheless, there are still many clinical difficulties due to the intricacy and diversity of root canal systems, especially in mandibular molars.[1] Early research by Hess and Zurcher revealed that root canal systems are highly irregular and intricate.[2] Multiple apical foramina, isthmuses, fins, apical deltas, intercanal connections, loops, and auxiliary canals are just a few of the anatomical features that make up the canal system and emphasise the complex internal morphology of teeth.[3] The middle mesial canal (MMC), a tiny and secretive canal situated between the mesiobuccal (MB) and mesiolingual (ML), is one of the anatomical differences that is most commonly overlooked. Mandibular molar canals.[4] Missed canals are a leading cause of endodontic failure, often resulting in persistent infection, apical periodontitis, and the need for retreatment. [2]
Usually, mandibular first molars have three canals and two roots. However, the presence of a fourth canal—the MMC—has been reported in the literature with a variable incidence ranging from 0.95% to 15%[5],[6]. The first reported cases of the mid-mesial canal (MMC) were documented by Barker et al. in 1969, followed by Vertucci in 1974.[4] Pomeranz et al. later classified MMCs into three types: fin, confluent, and independent canals, based on their configuration and relationship with the main mesial canals.[7]
Because of its thin and occasionally calcified character, the MMC is usually invisible on standard radiographs and arises from the pulpal floor between the MB and ML canals.[4] However, advanced diagnostic tools such as CBCT have aided in better detection of additional canals.[8] The capacity and precision of the practitioner to identify and treat such canals has been greatly improved by more recent technologies such as dental operating microscopes (DOM) and ultrasonic devices.[9]
This report emphasizes the importance of meticulous canal exploration, magnification, and the use of modern endodontic technology and advanced materials in identifying and treating middle mesial canals to prevent treatment failures and improve prognosis.
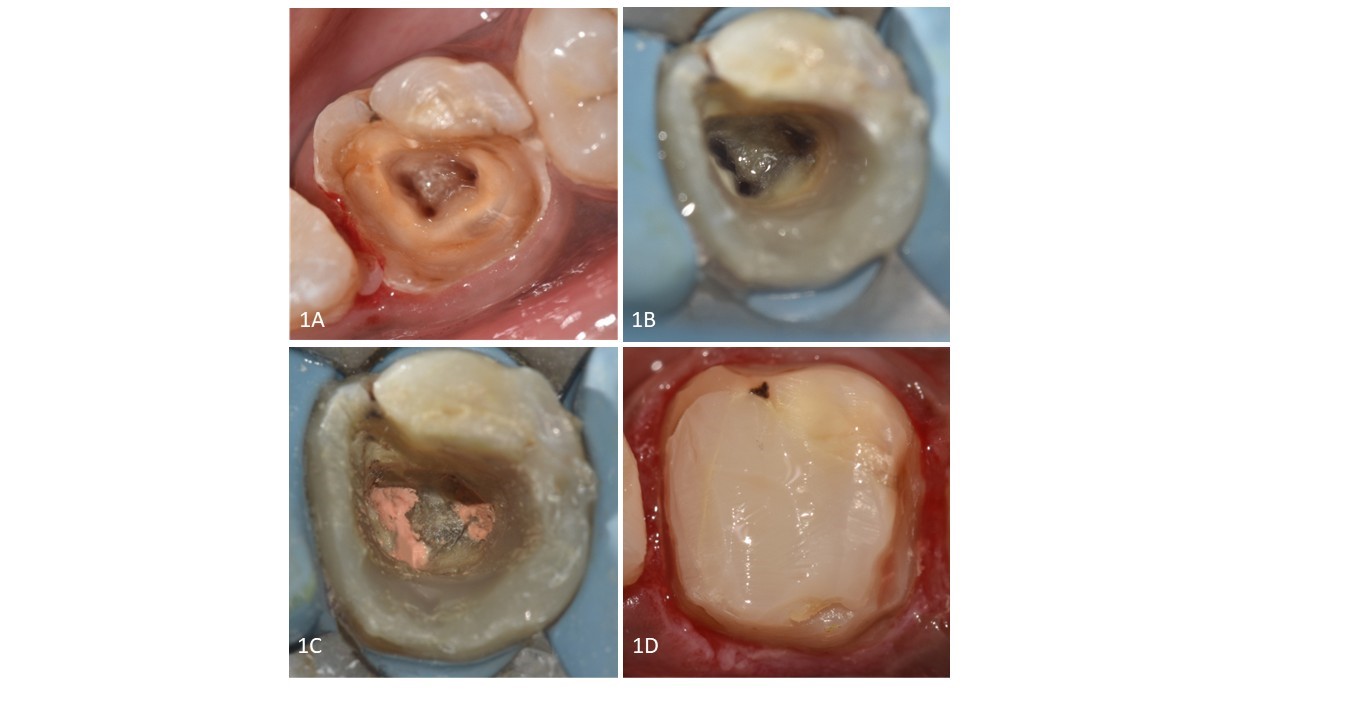
The main complaints of a 26-year-old female patient were food impact and tooth decay in the bottom left posterior area of the mouth. Intraoral examination showed deep dental caries on tooth #36 (mandibular left first molar), which was tender to percussion but showed no response to thermal sensitivity testing. The periapical radiograph demonstrated periodontal ligament widening, with no definitive radiographic indication of an additional mesial canal Figure 1A.
A diagnosis of pulpal necrosis with symptomatic apical periodontitis was made based on clinical and radiographic data.
Before beginning therapy, the patient was informed of the process, and their consent was duly obtained. In order to perform inferior alveolar nerve block (IANB), Lignox 2% (2% lignocaine with 1:80,000 adrenaline) was used.Dental caries was excavated and access-cavity preparation was done, and rubber dam (M care) isolation was obtained following the pre-endodontic buildup. Figure 2A, 2B
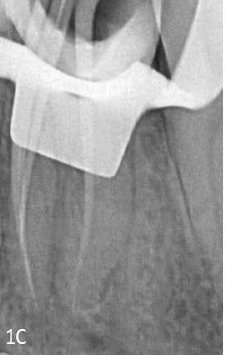
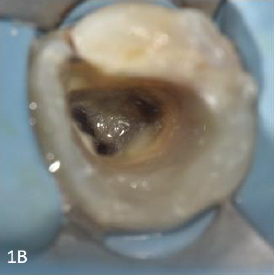
5.25% NaOCl (Vishal Dentocare, Signel Biomedical PVT. LTD.) was used to cleanse the pulp chamber. The dentinal map revealed the existence of one canal orifice in the distal root, two distinct separate canal orifices in the mesial root, and an additional dentinal groove between the two mesial orifices after a careful examination of the pulp chamber floor under 0.6X magnification (Laboured DNT Prima, USA). DG 16, when maneuvered in between both mesial orifices, confirmed the presence of an additional orifice, the middle mesial orifice. The midmesial orifice was troughed using a golden tip with Ultra X (Eighteeth, Orikam). Using an electronic apex locater (Eighteeth, Orikam), the working length was calculated using an ISO 15 K file (MANI, Japan) and validated radiographically Fig 1B. The canal patency was evaluated using an ISO 10 K file (MANI, Japan).
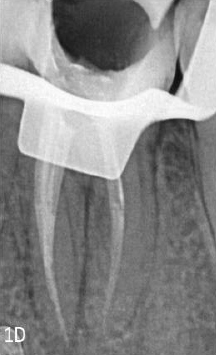
To verify the middle mesial canal's direction, the radiograph was taken in angulation. In addition to 5.25% NaOCl copious irrigation in between the instrumentation, all of the canals were instrumented using the Neoendo Flex (Orikam, India) system up to size 25/4% in mesial canals and 25/6% in distal canals. A digital periapical radiograph was used to verify and validate the master cone fit Figure 1C. The canals were obturated with gutta-percha cones coated with AH Plus sealer (Dentsply, Switzerland), Figure 1D followed by short fiber reinforced composite (Everex Posterior, GC) and bulkfill composite (Charisma, Kultzer) for post endodontic restoration in the same visit.Figure 1E, Figure 2D,






Various methods have been employed to assess anatomical variations in root canal systems, such as cross-sectional analysis, canal clearing techniques, clinical exploration, and advanced imaging modalities [10]. However, many of these techniques are confined to research settings and are not feasible for routine clinical use. As a result, radiographic evaluation remains the primary and most practical diagnostic tool available to clinicians for assessing root canal morphology during endodontic treatment [11]. While conventional intraoral periapical radiographs are a crucial tool in endodontic procedures, their two-dimensional nature limits their ability to fully reveal complex canal morphology [12]. The identification of the middle mesial canal can be challenging due to its narrow or calcified nature and thus often goes unnoticed and undetected in diagnostic radiographic evaluation [4].
A well-flared access cavity is essential for optimal visualization of the pulpal chamber anatomy [13]. Inadequate or constricted access may hinder visibility, increasing the risk of overlooking canals such as the mesiobuccal or mesiolingual. The dental operating microscope (DOM) provides significant advantages by enhancing illumination and offering superior visualization. It allows the clinician to detect subtle color changes, facilitates accurate interpretation of the dentinal floor anatomy, and enables the precise placement of fine instruments through high magnification and coaxial lighting [9]. Additionally, ultrasonic troughing enhances tactile sensitivity and plays a crucial role in locating and accessing additional canals. It overcomes the limitations posed by traditional handpieces, which can obscure visibility during canal exploration [14].
Sherwani et al. (2016) [15] reported that in the Indian population, 67% of MMC orifices were located between the MB and ML canals, 20% closer to ML, and 12% nearer to MB . Similarly, Soares De et al. (2012) [16] found the MMC orifice was closest to MB in 46% of cases, ML in 31%, and centrally positioned in 23% . The MMC orifice in this instance was situated nearer the MB canal.
Pomeranz et al. (1980) [7] categorized MMCs into three types: fin, confluent, and independent. In this case, the MMC was of the confluent type, joining the MB canal apically The middle mesial canal combines with the mesiobuccal canal in 44.5% of cases and with the mesiolingual canal in 14.8% of cases at the apical region.
To ensure. In this instance, the mesiobuccal canal and the middle mesial canal met. Failure to treat all canals, especially additional ones like MMCs, can result in persistent infection, as microorganisms may remain in untreated spaces [17]. Early identification and proper instrumentation of such anatomy significantly improve progonosis. All root canals must be appropriately formed, cleaned, and accessible in order to guaruantee a hermetic seal throughout the system [18]. The root canal preparation was done with Neoendo Flex. The teeth were instrumented with Neoendo Flex (Orikam, India) files as instructed by the manufacturer, operating at 350 RPM and 1.5 Ncm torque [19]. NeoEndo Flex files have undergone gold thermal treatment, enhancing their flexibility and cutting efficiency, which are critical factors in successful root canal procedures [20]. The obturation was completed with Neoendo GP with AH Plus sealer. Figure 1D Because of its dimensional stability and resistance to resorption, AH plus sealer has been regarded as the gold standard for sealers in research [21].
The quality of the coronal restoration is even more crucial to the success of endodontically treated teeth (ETT) than successful root canal therapy. Since in this case only the distobuccal wall was remaining, rehabilitation and adequate buildup of post-endodontic restoration was of utmost importance.
Since it has been demonstrated to have greater fracture resistance, short- fiber reinforced composite (Everex Posterior, GC) was selected for the project. The composite strengthened with short fibres was further repaired using bulkfill composite (Kulzer, Charisma) [22].
In order to improve the long-term prognosis of endodontic therapy, clinicians should be urged to carefully inspect the pulp chamber floor for any new canal orifices.
As a patient undergoing endodontic treatment for my mandibular left first molar, I must say the experience was both reassuring and a bit overwhelming. Initially, I was quite concerned because I had deep cavities and felt tenderness in the tooth. However, when I visited the clinic, the dentist explained everything in detail, which helped calm my nerves. The advanced technology, like the dental operating microscope (DOM), was used to carefully examine my tooth, which gave me confidence in the process.
What stood out to me was that the dentist found an additional canal, the middle mesial canal (MMC), which hadn’t been visible on the initial radiographs. I was impressed with the precision and thoroughness the team displayed in identifying this hidden canal, as it could have easily been overlooked. I appreciated how the dentist explained each step of the procedure, from caries excavation to canal cleaning and obturation, making sure I understood everything being done.
Throughout the procedure, I felt no pain thanks to the anesthesia. I left the clinic feeling optimistic and relieved, knowing that the dental team had taken every precaution to ensure a successful treatment and long-term health of my tooth.
This case emphasizes the use of a meticulous approach and the use of magnification, ultrasonics in locating anatomical variations such as the middle mesial canal. To increase the success rate of endodontic therapy, a thorough understanding of tooth shape is essential.Clinicians should maintain a high index of suspicion, especially in mandibular first molars, to ensure comprehensive endodontic therapy and avoid missed canals that could compromise treatment outcomes.